The patient presents with community-acquired urosepsis from E. coli. The resistance pattern is key: resistant to ampicillin and first-generation cephalosporins (cephalothin), but susceptible to third-generation cephalosporins (ceftriaxone) and fluoroquinolones. ESBL is negative, ruling out extended-spectrum beta-lactamase.
E. coli carries a chromosomal ampC gene that encodes an AmpC-type beta-lactamase. Under normal conditions, this gene is repressed by the ampD gene product. However, mutations in the ampC promoter region (or loss of ampD function) lead to constitutive, high-level expression of AmpC.
AmpC beta-lactamases:
PBP mutations cause broad resistance to all beta-lactams, including third-generation cephalosporins. This patient is susceptible to ceftriaxone, so PBP mutation is unlikely. PBP mutations are also rare in E. coli (more common in S. pneumoniae and N. gonorrhoeae).
While plasmid-mediated AmpC (pAmpC) exists and can be found in E. coli, it is far less common than chromosomal AmpC derepression in community-acquired infections. The clinical presentation (urosepsis, likely community-acquired) and the absence of ESBL make chromosomal AmpC derepression the most likely mechanism. Additionally, plasmid-mediated AmpC is more commonly associated with Klebsiella and other Enterobacteriaceae in healthcare settings.
Outer membrane porin mutations reduce beta-lactam penetration but do NOT cause the specific resistance pattern seen here. OmpF loss would cause resistance to multiple drug classes and would not explain the selective susceptibility to ceftriaxone. This mechanism is also rare in E. coli and more relevant in Pseudomonas aeruginosa.
AmpC beta-lactamases and their genetic basis are covered in detail in standard microbiology references. The distinction between ESBL and AmpC is a high-yield topic for NEET PG because it directly impacts antibiotic selection in clinical practice.
Loading illustration…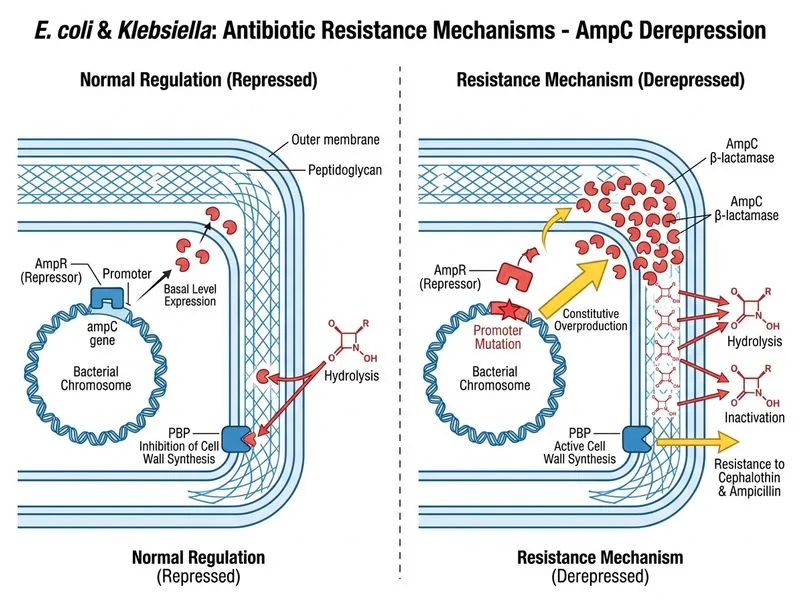
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →