A 72-year-old woman from Mumbai presents with palpitations and dizziness for 30 minutes. She denies chest pain. Vital signs: BP 110/68 mmHg, HR 165 bpm (irregular), RR 20/min. On auscultation, the heart sounds are irregularly irregular. Her ECG shows a ventricular rate of 160–180 bpm with no discernible P waves, and the baseline appears to have a fine, irregular undulation. Her troponin is normal. What is the most likely diagnosis?
A. Atrial flutter with rapid ventricular response
B. Supraventricular tachycardia with aberrant conduction
C. Atrial fibrillation with rapid ventricular response
D. Ventricular tachycardia
Explanation
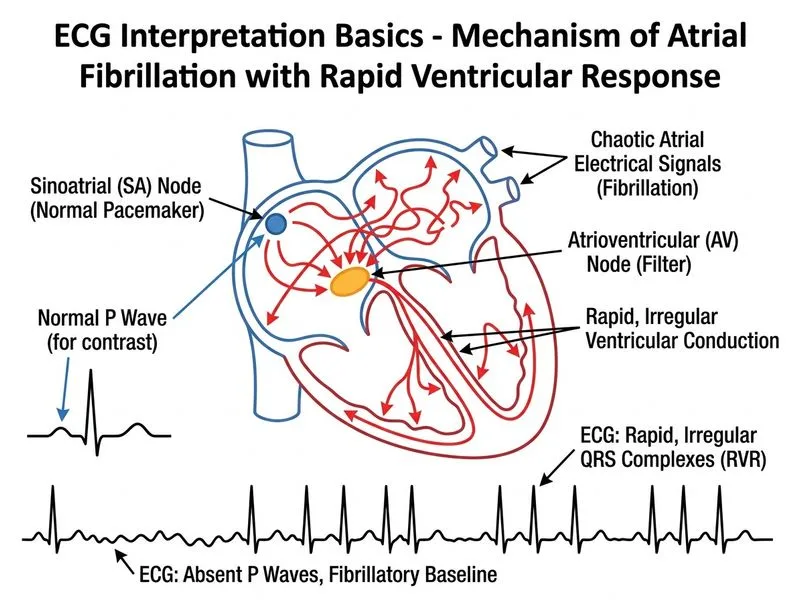
Atrial Fibrillation: ECG Recognition and Clinical Correlation
Key ECG Findings in This Case
Key Point
The combination of an irregularly irregular heart rhythm, absence of P waves, and fine baseline undulation (fibrillatory waves or "f waves") is diagnostic of atrial fibrillation (AF).
Differential Diagnosis of Rapid Arrhythmias
Table
Feature
Atrial Fibrillation
Atrial Flutter
Ventricular Tachycardia
SVT
Rhythm
Irregularly irregular
Regular (or regular with variable block)
Regular
Regular
P waves
Absent; replaced by f waves
Sawtooth pattern (flutter waves)
Absent or buried
Buried in QRS/T
Baseline
Fine or coarse fibrillatory waves
Sawtooth baseline
Smooth
Smooth
QRS duration
Narrow (< 120 ms) unless aberrancy
Narrow
Wide (≥ 120 ms)
Narrow
Ventricular rate
100–180 bpm (uncontrolled)
150–350 bpm
120–250 bpm
140–250 bpm
Heart sounds
Irregularly irregular
Regular or regular with pauses
Regular
Regular
Clinical Pearl
The irregularly irregular rhythm is the hallmark of AF. When you hear the heart sounds are "irregularly irregular," AF should be your first thought. This distinguishes AF from atrial flutter, which typically presents with a regular ventricular response (unless variable AV block is present).
Pathophysiology of Atrial Fibrillation
1.
Loss of organized atrial contraction → multiple ectopic foci fire chaotically in the atria
2.
Fibrillatory waves replace normal P waves (fine waves at ~350–600 bpm)
3.
Variable AV nodal conduction → irregular ventricular rate (typically 100–180 bpm if uncontrolled)
4.
Loss of atrial kick → reduced cardiac output and increased stroke volume variability
Clinical Features in This Patient
Palpitations and dizziness → due to rapid, irregular ventricular rate and loss of atrial contribution to ventricular filling
Irregularly irregular pulse → pathognomonic for AF
Normal troponin → rules out acute MI; AF can be primary (lone AF) or secondary to other cardiac/systemic conditions
No chest pain → suggests AF is not secondary to acute coronary syndrome
High-YieldNEET PG
AF is the most common sustained arrhythmia in clinical practice. Risk factors include:
Age > 65 years
Hypertension
Heart failure
Valvular disease
Hyperthyroidism
Chronic lung disease
Diabetes
Management Approach
Loading diagram...
Mnemonic: AF = CHADS2VASc Score for Stroke Risk
Congestive heart failure
Hypertension
Age ≥ 75 years (2 points)
Diabetes
Stroke/TIA/thromboembolism (2 points)
Vascular disease
Age 65–74 years
Sex category (female)
clinical category
Score ≥ 2 in men or ≥ 3 in women → anticoagulation indicated.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.