Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
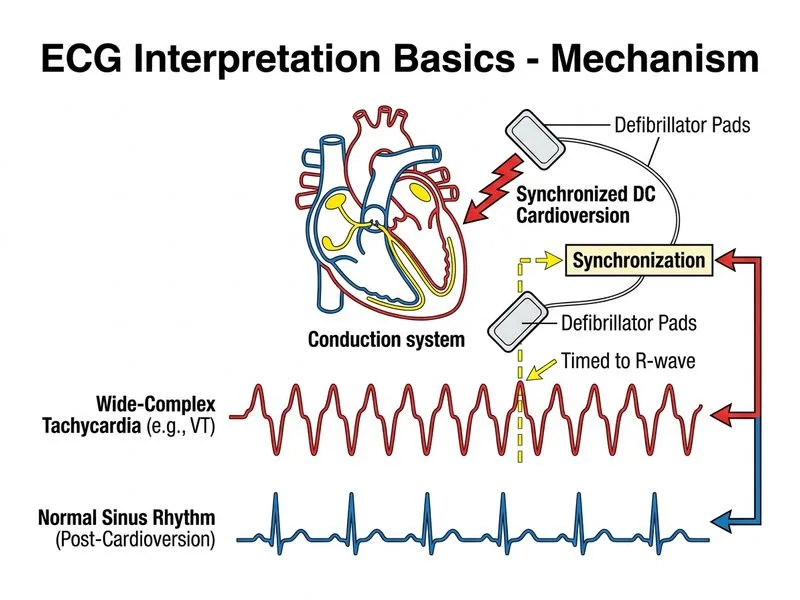
Join on Telegram →This patient presents with a regular wide-complex tachycardia (WCT) at 160 bpm with 2:1 AV block. The combination of:
...is highly suggestive of atrial flutter with fixed 2:1 AV conduction or atrial tachycardia with AV block, both of which are refractory to adenosine and calcium channel blockers because the arrhythmia originates above the AV node but the AV node is not the rate-limiting structure.
2:1 AV conduction block in a regular WCT indicates the arrhythmia is NOT AV-node-dependent. Adenosine and calcium channel blockers work by blocking AV nodal conduction; they will not terminate arrhythmias where the AV node is merely a passive bystander. In this hemodynamically stable patient, synchronized DC cardioversion is the definitive treatment.
| Feature | Adenosine/Verapamil Effective? | Reason |
|---|---|---|
| AVNRT / AVRT | ✓ Yes | AV node is part of reentrant circuit |
| Atrial flutter with 2:1 block | ✗ No | AV node is not the arrhythmia source |
| Atrial tachycardia with block | ✗ No | Ectopic atrial focus; AV block is passive |
| Ventricular tachycardia | ✗ No | Originates below AV node |
The 2:1 AV conduction ratio is a clue to atrial flutter. In atrial flutter, the atrial rate is typically 250–350 bpm; the AV node conducts every other impulse (2:1 block) by default, resulting in a ventricular rate of 125–175 bpm. This is a classic ECG pattern and should trigger immediate recognition that adenosine will not work.
Adenosine is the first-line drug for all regular WCT — this is a common misconception. Adenosine is first-line only for AV-node-dependent arrhythmias (AVNRT, AVRT). For atrial flutter, atrial tachycardia, and VT, adenosine either has no effect or may transiently increase AV block without terminating the arrhythmia, wasting time.
Verapamil is safe in all WCT — verapamil is contraindicated in VT and can cause hemodynamic collapse. In this case, even if VT were suspected, verapamil would be dangerous.
Since the patient is hemodynamically stable, sedation is appropriate before cardioversion. Synchronized DC cardioversion at 100–200 J is the gold standard for terminating atrial flutter and other AV-node-independent arrhythmias.
Harrison 21e Ch 296; Braunwald's Heart Disease 12e Ch 36
Loading illustration…