| Feature | Acute MI | LVH |
|---|---|---|
| ST-segment elevation | Present (acute transmural injury) | Absent |
| Reciprocal ST depression | Yes (in non-infarcted territory) | No |
| QRS voltage | May be normal or low | Increased (Sokolow-Lyon, Cornell criteria) |
| T-wave changes | Symmetrical inversion (acute phase) | Asymmetrical inversion (strain pattern) |
| Onset | Acute (hours) | Gradual (months to years) |
| Evolutionary pattern | Dynamic (ST→T changes over days) | Static |
Harrison 21e Ch 297
Loading illustration…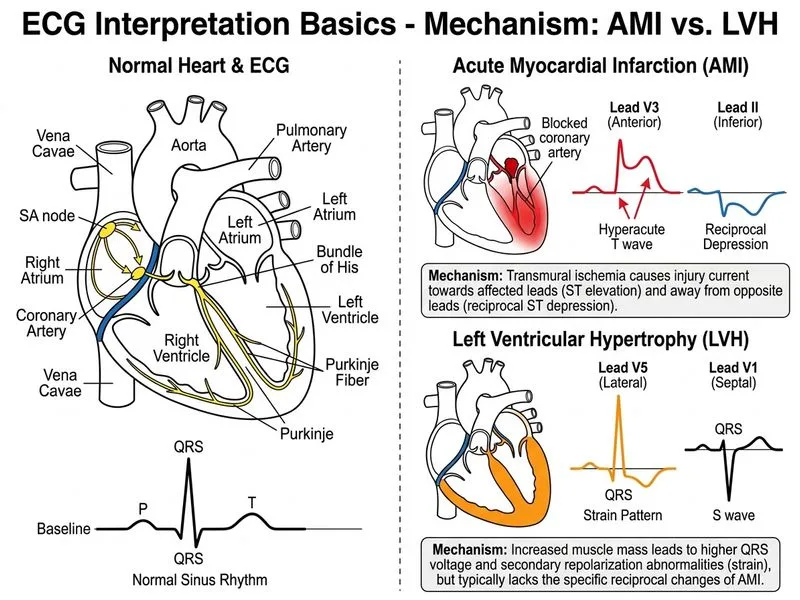
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →