A 52-year-old man from Delhi presents to the emergency department with acute onset chest pain radiating to the left arm for 2 hours. He is diaphoretic and anxious. Vital signs: BP 128/82 mmHg, HR 102/min, RR 18/min. His ECG shows ST-segment elevation in leads II, III, and aVF with reciprocal ST depression in leads I and aVL. The PR interval measures 0.16 seconds, QRS duration 0.08 seconds, and QT interval 0.38 seconds. What is the primary abnormality indicated by the ST-segment changes?
A. Acute anterior wall myocardial infarction due to left anterior descending artery occlusion
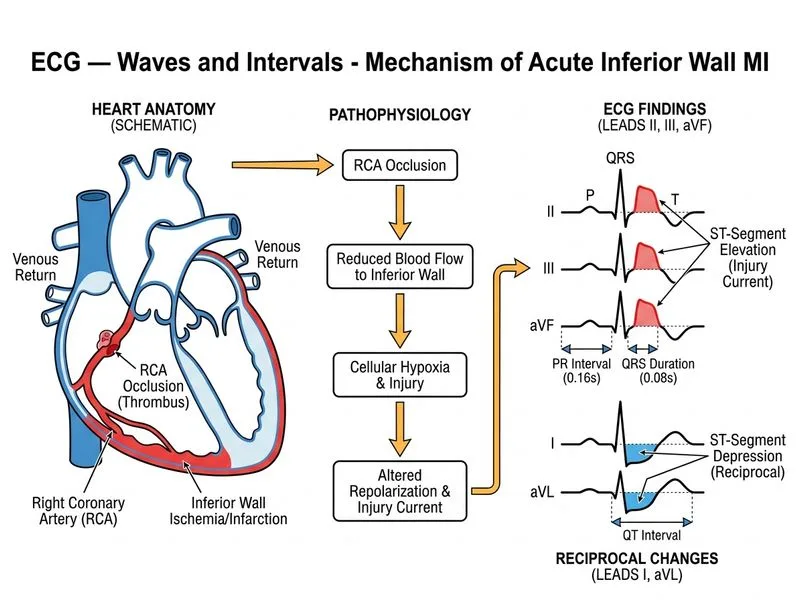
B. Acute inferior wall myocardial infarction due to right coronary artery occlusion
C. Acute left ventricular hypertrophy with secondary ST changes
Acute pericarditis with diffuse ST-segment elevation
D.
Explanation
Clinical Presentation and ECG Interpretation
Key Point
ST-segment elevation in the inferior leads (II, III, aVF) with reciprocal ST depression in the lateral leads (I, aVL) is pathognomonic for acute inferior wall myocardial infarction (IWMI).
Anatomical Localization
The inferior wall of the left ventricle is primarily supplied by the right coronary artery (RCA) in approximately 80% of the population. The ECG pattern of inferior STEMI is:
Table
Lead Group
Finding
Interpretation
II, III, aVF
ST elevation
Inferior wall infarction
I, aVL
ST depression
Reciprocal changes
V1–V3
Normal or depression
Excludes anterior STEMI
Normal ECG Intervals in This Patient
High-YieldNEET PG
The PR interval (0.16 s), QRS duration (0.08 s), and QT interval (0.38 s) are all within normal limits:
PR interval: 0.12–0.20 seconds ✓
QRS duration: 0.06–0.10 seconds ✓
QT interval: corrected QT (QTc) = 0.38 s (normal for HR ~102) ✓
These normal intervals rule out conduction abnormalities or prolongation that might suggest alternative diagnoses.
Pathophysiology of STEMI
1.
Acute coronary occlusion → transmural ischemia
2.
Loss of repolarization voltage in infarcted zone
3.
Current of injury flows from viable to infarcted tissue
4.
Epicardial leads over infarct zone → ST elevation
5.
Reciprocal leads → ST depression (opposite vector)
Clinical Pearl
Inferior STEMI carries a lower in-hospital mortality (3–5%) compared to anterior STEMI (5–10%), but right ventricular involvement (present in ~30% of inferior STEMI) can cause hemodynamic collapse if not recognized early.