ECG — Waves and Intervals MCQ — NEET PG Practice Question | NEETPGAI
ECG — Waves and Intervals
medium
heart-pulse Physiology
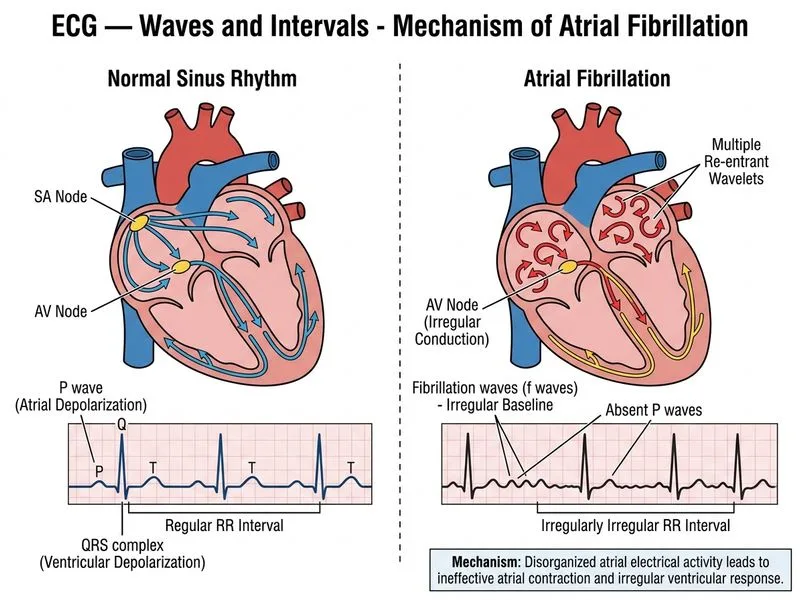
A 68-year-old woman from Mumbai presents with palpitations and lightheadedness for 3 days. She has a history of hypertension and atrial fibrillation. On examination, her pulse is irregularly irregular at 110/min, BP 138/88 mmHg. A 12-lead ECG is obtained. The ECG shows absent P waves, an irregular ventricular rate of 100–130/min, and a QRS duration of 0.09 seconds. The RR intervals vary from 0.35 to 0.65 seconds. Which of the following ECG findings is most characteristic of her rhythm?
A. Delta waves with short PR interval and wide QRS complexes
B. Regular P waves at a rate of 150/min with variable AV conduction and fixed PR intervals
C. Presence of fibrillation waves (f waves) with irregular baseline and absence of distinct P waves
D. Narrow QRS complexes with a regular rate and sawtooth pattern in the baseline
Explanation
Atrial Fibrillation: ECG Diagnosis and Pathophysiology
Key Point
Atrial fibrillation (AF) is characterized by absence of organized P waves and replacement by fine or coarse fibrillation waves (f waves) with an irregularly irregular ventricular response.
ECG Hallmarks of Atrial Fibrillation
Table
ECG Feature
Finding in AF
Significance
P waves
Absent; replaced by f waves
Loss of organized atrial depolarization
Fibrillation waves (f waves)
Fine (amplitude <0.5 mm) or coarse (>0.5 mm)
Chaotic atrial electrical activity
Baseline
Irregular, undulating
No isoelectric line between QRS complexes
Ventricular rate
Irregularly irregular (100–180/min untreated)
Variable AV nodal conduction
QRS duration
0.06–0.10 seconds (narrow)
Supraventricular origin
RR intervals
Variable (no fixed pattern)
Hallmark of irregularly irregular rhythm
Pathophysiology of AF
Loading diagram...
High-YieldNEET PG
The irregularly irregular rhythm is the clinical hallmark — no two consecutive RR intervals are identical. This distinguishes AF from other arrhythmias like atrial flutter (regular) or premature beats (occasional irregularity).
Why Fibrillation Waves Appear
1.
Atrial myocardium depolarizes at multiple sites simultaneously
2.
No organized P wave can form (normal P wave requires sequential atrial activation)
3.
Baseline shows continuous, chaotic electrical activity → f waves
4.
Amplitude of f waves varies:
Coarse f waves (>0.5 mm): easier to see, more organized atrial activity
Fine f waves (<0.5 mm): may appear as flat baseline, more disorganized
Clinical Pearl
Fine f waves can be mistaken for a flat baseline; careful inspection of the baseline between QRS complexes is essential. If unsure, lead V1 often shows f waves more clearly.
Clinical Significance in This Patient
Mnemonic: CHADS₂-VASc — scoring system for stroke risk in AF:
Congestive heart failure
Hypertension (present in this patient)
Age ≥75 years (or 65–74 with 1 point)
Diabetes
Stroke/TIA/thromboembolism (2 points)
Vascular disease
Age 65–74
Scex category (female)
This patient (age 68, hypertension) has a CHADS₂-VASc score of ≥2, indicating need for anticoagulation (warfarin or DOAC) in addition to rate control.
Management Approach
Warning
Do NOT confuse AF with atrial flutter:
Atrial flutter: Regular atrial rate (250–350/min), sawtooth P waves, regular ventricular rate (if fixed AV block)