The patient presents with an incidental finding of prolonged QTc interval (normal: < 450 ms in women). The differential diagnosis of prolonged QT includes:
The asymptomatic status and absence of family history do not exclude either category, but the investigation strategy must first exclude reversible, life-threatening acquired causes before pursuing genetic testing.
Mnemonic: ABCDE of QT Prolongation —
| Investigation | Indication | Timing |
|---|---|---|
| Electrolyte panel | All patients with prolonged QT | First — immediate |
| Medication review | All patients with prolonged QT | First — concurrent |
| Genetic testing | Persistent QT prolongation after electrolyte/drug correction; family history of sudden death; recurrent syncope | Third — after acquired causes excluded |
| Exercise stress test | Suspected LQTS (especially Romano-Ward type); syncope with exercise | Selective — if LQTS suspected |
| Coronary angiography | Chest pain or ischemic ECG changes | Not indicated for QT prolongation alone |
In this asymptomatic woman with incidental QT prolongation, the absence of syncope or family history does not exclude congenital LQTS, but it does lower pretest probability. Electrolyte correction is the critical first step: if QTc normalizes after electrolyte repletion, no further workup may be needed. If QTc remains prolonged despite normal electrolytes and no offending drugs, genetic testing becomes appropriate.
Loading illustration…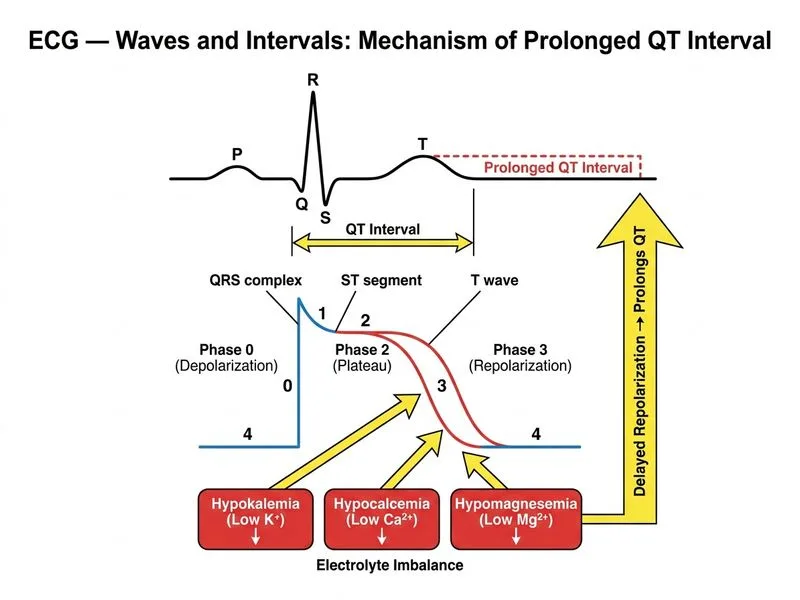
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →