ECG — Waves and Intervals MCQ — NEET PG Practice Question | NEETPGAI
ECG — Waves and Intervals
medium
heart-pulse Physiology
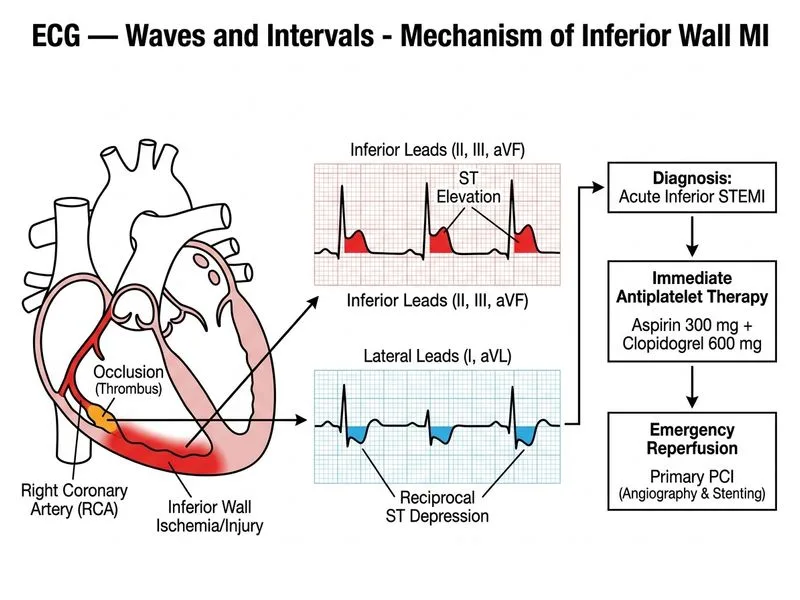
A 58-year-old man from Delhi presents to the emergency department with acute onset chest pain radiating to the left arm for 2 hours. His ECG shows ST elevation in leads II, III, and aVF with reciprocal ST depression in leads I and aVL. His troponin I is elevated at 2.8 ng/mL (normal <0.04). Blood pressure is 95/60 mmHg, heart rate 58 bpm, and he is diaphoretic. What is the most appropriate immediate next step in management?
A. Start intravenous heparin, observe for 6 hours, and perform stress testing if symptoms resolve
B. Administer aspirin 300 mg, clopidogrel 600 mg, and arrange emergency coronary angiography with primary PCI
C. Obtain a repeat ECG in 15 minutes and measure serial troponins before deciding on intervention
Administer thrombolytic therapy (streptokinase) and defer angiography to day 3
D.
Explanation
Clinical Scenario Analysis
This patient presents with acute ST-elevation myocardial infarction (STEMI) of the inferior wall (ST elevation in II, III, aVF indicates right coronary artery occlusion). The combination of acute chest pain, elevated troponin, hemodynamic compromise (hypotension, bradycardia), and diagnostic ECG changes mandates immediate reperfusion therapy.
Reperfusion Strategy in STEMI
Key Point
In a PCI-capable centre (which Delhi hospitals are), primary PCI is the gold standard for STEMI with a door-to-balloon time target of ≤90 minutes. This patient requires urgent coronary angiography to identify the culprit lesion and restore flow.
High-YieldNEET PG
The inferior STEMI with bradycardia and hypotension raises concern for right ventricular (RV) infarction. RV infarcts are preload-dependent; fluid resuscitation may be needed, but this does not delay PCI.
Why Option 0 Is Correct
1.
Dual antiplatelet therapy (aspirin + clopidogrel loading) is guideline-mandated before PCI in STEMI.
2.
Emergency coronary angiography with primary PCI is the definitive reperfusion method in a PCI-capable hospital.
3.
Time is myocardium: every minute of delay increases mortality and infarct size.
4.
Hemodynamic instability (SBP 95 mmHg) is NOT a contraindication to PCI; it is an indication for urgent intervention.
Loading diagram...
Inferior STEMI with RV Involvement
Table
Feature
Inferior STEMI
RV Infarction (Complication)
ST elevation
II, III, aVF
Also in V4R (right-sided ECG)
Hemodynamics
Normal or mild ↓ BP
Marked ↓ BP, ↑ JVP (preload-dependent)
Management
Standard PCI + fluids as needed
Avoid nitrates; fluid resuscitation; PCI still indicated
Bradycardia
Common (vagal)
Common (RV ischemia)
Clinical Pearl
Do NOT delay PCI to obtain a right-sided ECG (V4R) in suspected RV infarction. The diagnosis is clinical (hypotension + inferior STEMI + elevated JVP), and PCI is still the definitive treatment.
Warning
Thrombolytic therapy is slower, less effective, and carries higher re-infarction risk than primary PCI in a PCI-capable centre. It is reserved for PCI-incapable hospitals or when PCI cannot be performed within 120 minutes of first medical contact.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.