ECG — Waves and Intervals MCQ — NEET PG Practice Question | NEETPGAI
ECG — Waves and Intervals
medium
heart-pulse Physiology
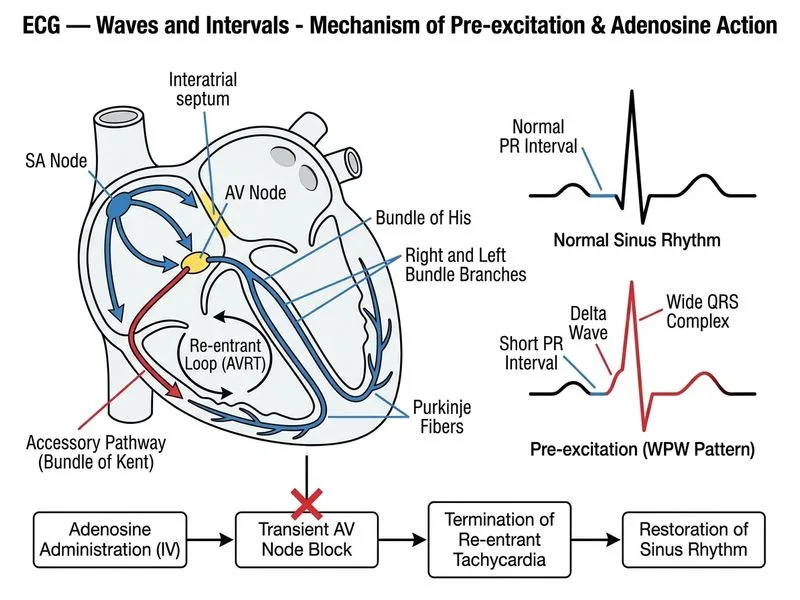
A 72-year-old woman from Mumbai is admitted with palpitations and dyspnea. Her ECG shows a regular narrow-complex tachycardia at 160 bpm with a PR interval of 0.08 seconds (short PR) and a slurred upstroke (delta wave) in the QRS complex. She is hemodynamically stable. What is the most appropriate immediate next step in management?
A. Perform synchronized DC cardioversion under sedation
B. Start oral verapamil 80 mg and observe for response
C. Obtain an electrophysiology study to confirm the diagnosis and plan ablation
D. Administer intravenous adenosine 6 mg rapid push followed by saline flush
Explanation
ECG Diagnosis: Wolff-Parkinson-White (WPW) Syndrome with Atrioventricular Reentrant Tachycardia (AVNRT)
Key Point
The short PR interval (<0.12 s) and delta wave (slurred QRS upstroke) are pathognomonic for pre-excitation via an accessory pathway (AP). In the setting of a regular narrow-complex tachycardia, this is AVNRT in WPW syndrome.
High-YieldNEET PG
WPW-associated AVNRT is the most common tachyarrhythmia in patients with pre-excitation. The reentry circuit uses the AV node (orthodromic) and the AP (antidromic) in a reciprocal loop.
Acute Management of Hemodynamically Stable AVNRT in WPW
First-Line Agent: Adenosine
Mechanism: Adenosine blocks AV nodal conduction, breaking the reentry circuit by interrupting the orthodromic limb of the circuit.
Dosing:
Initial: 6 mg IV rapid push followed by 10–20 mL saline flush
If no response in 1–2 minutes: 12 mg IV rapid push
Success rate: >90% for AVNRT termination
Clinical Pearl
Adenosine works rapidly (within seconds) and is safe even in the elderly because its half-life is <10 seconds. Transient asystole or brief hypotension is expected and self-limited.
Warning
Verapamil is contraindicated in pre-excited atrial fibrillation (AF with WPW) because it blocks the AV node preferentially, forcing conduction down the AP, which may have a shorter refractory period and cause rapid ventricular rates or degeneration to VF. However, in orthodromic AVNRT (narrow-complex), verapamil is theoretically safe but is second-line because adenosine is faster and more reliable.
Loading diagram...
Why Other Options Are Suboptimal
Table
Option
Reason
DC Cardioversion
Reserved for hemodynamic instability or adenosine failure. This patient is stable and adenosine is first-line.
Verapamil
Second-line agent; slower onset than adenosine. Also carries risk in pre-excited AF (though not relevant here).
EP Study
Diagnostic and therapeutic (ablation) but NOT an acute management step. EP study is arranged after acute termination and stabilization.
High-YieldNEET PG
The short PR interval persists even when the tachycardia is terminated (it is a baseline feature of WPW). Do not mistake resolution of tachycardia for resolution of pre-excitation; the AP remains and requires definitive ablation.
Definitive Management
After acute termination:
1.
Electrophysiology study to localize the AP
2.
Radiofrequency catheter ablation of the AP (curative; >95% success)
3.
Avoid long-term rate-limiting drugs (beta-blockers, verapamil) in pre-excited AF because they increase AP conduction risk
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.