Fracture Classification — Types and Patterns MCQ — NEET PG Practice Question | NEETPGAI
Fracture Classification — Types and Patterns
medium
bone Orthopedics
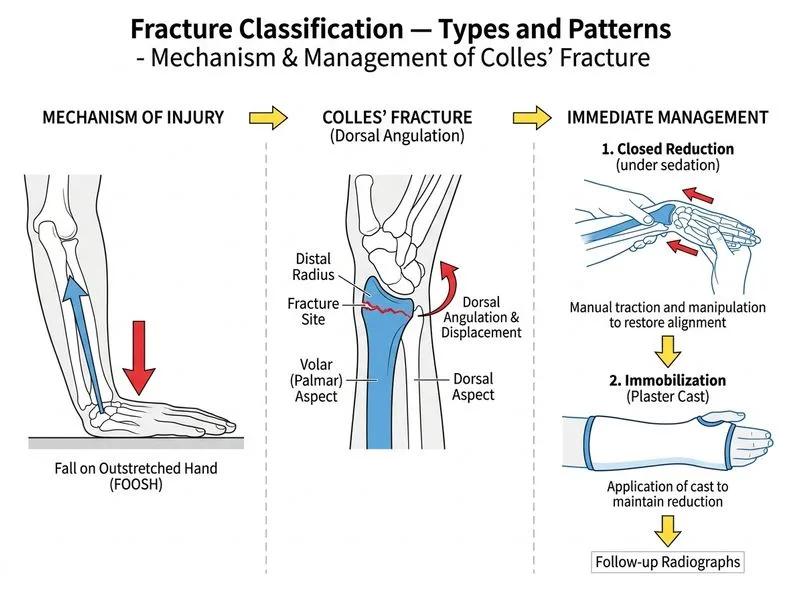
A 28-year-old woman falls on an outstretched hand while playing badminton. She presents with wrist pain, swelling over the dorsal aspect of the wrist, and a 'dinner fork' deformity. Plain radiographs confirm a Colles' fracture with dorsal angulation of 35° and dorsal displacement. She has no neurovascular compromise. What is the most appropriate immediate next step in management?
A. Apply a sling and refer for physiotherapy after 2 weeks
B. Obtain a CT scan to assess intra-articular extension before any intervention
C. Perform closed reduction under procedural sedation followed by immobilization in a plaster cast
D. Arrange for open reduction and internal fixation with plate and screws
Explanation
Clinical Scenario
This is a classic Colles' fracture (distal radius fracture with dorsal angulation and displacement) in a young, active patient with no neurovascular compromise. The 'dinner fork' deformity is pathognomonic.
Why Closed Reduction is the Correct First Step
Key Point
Colles' fractures are initially managed by closed reduction under procedural sedation (propofol, midazolam, or nitrous oxide) followed by immobilization in a plaster cast. This is the gold standard for uncomplicated, non-comminuted fractures in patients with intact neurovascular status.
High-YieldNEET PG
The Lister's tubercle is the key anatomical landmark for reduction:
Dorsal angulation > 20° or displacement > 5 mm requires reduction
This patient's 35° angulation is well above the threshold
Reduction Technique (Colles' Fracture)
Table
Step
Technique
Goal
Analgesia
Procedural sedation ± hematoma block
Pain control, muscle relaxation
Traction
Longitudinal pull on extended wrist
Restore length
Correction
Flex wrist, apply volar pressure
Correct dorsal angulation
Immobilization
Above-elbow plaster cast
Maintain reduction
Follow-up X-rays
At 1 week, 4 weeks, 8 weeks
Monitor for loss of reduction
Clinical Pearl
Colles' fractures are prone to loss of reduction in the first 2 weeks. Weekly X-rays are essential. If reduction is lost, consider percutaneous pinning or ORIF.
Mnemonic
COLLES = Closed reduction → Over-extension → Lateral (radial) displacement → Loss of volar tilt → Elevate → Stab with cast
When to Consider ORIF
Warning
Open reduction is reserved for:
Comminuted intra-articular fractures
Fractures with loss of reduction after closed reduction
Fractures in patients requiring early mobilization (athletes, elderly with osteoporosis)
Associated injuries (ulnar fracture with displacement, median nerve compression)
This patient has a simple displaced fracture without comminution — closed reduction is appropriate.
Rockwood & Green's Fractures in Adults Ch 10
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.