A 28-year-old female sustained a fracture of the distal radius 3 weeks ago. She complains of persistent pain and swelling at the fracture site. On examination, there is mild tenderness and some crepitus. The treating surgeon wants to assess whether soft callus formation has begun and to monitor the early stages of fracture healing before allowing mobilization.
A. Computed tomography scan
B. Plain radiography (posteroanterior and lateral views)
C. Magnetic resonance imaging
D. Radioisotope bone scan (technetium-99m)
Explanation
Investigation of Choice for Assessing Early Fracture Healing (Soft Callus Stage)
Why Plain Radiography is the First-Line Investigation
Key Point
Plain radiography (posteroanterior and lateral views) is the standard first-line investigation for monitoring fracture healing at all stages, including the soft callus stage at 2–3 weeks. It is readily available, cost-effective, and provides sufficient structural detail to assess callus formation and fracture alignment.
High-YieldNEET PG
At 3 weeks post-fracture, soft callus is typically becoming radiographically visible on plain films in uncomplicated fractures. Plain radiography allows the surgeon to assess bridging callus, fracture alignment, and early signs of union before permitting mobilization. This is the routine clinical approach as recommended in standard orthopedic practice (Rockwood & Green's Fractures in Adults).
Timeline of Radiological Visibility in Fracture Healing
Table
Investigation
Inflammatory Stage (0–3 days)
Soft Callus (2–3 weeks)
Hard Callus (3–8 weeks)
Remodeling (8 weeks+)
Plain Radiography
Fracture line visible
Soft callus becoming visible
Bridging callus clearly visible
Progressive mineralization
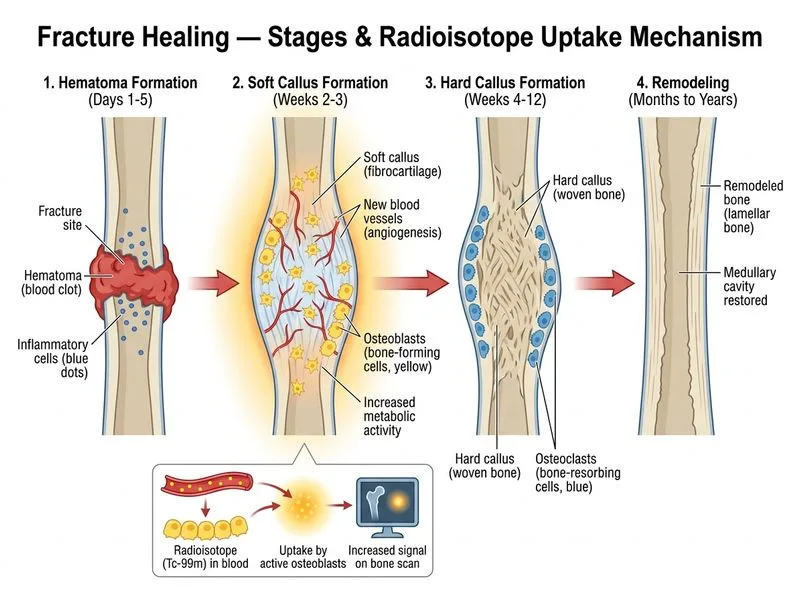
Radioisotope Scan
Positive (24–48 hrs)
Peak uptake
Moderate uptake
Decreasing uptake
MRI
Marrow edema visible
Soft tissue callus visible
Can assess union
Remodeling phase
CT Scan
Fracture line clear
Early callus may be seen
Hard callus clear
Detailed remodeling
Clinical Pearl
Plain radiography is the investigation of choice for routine monitoring of fracture healing at all stages. Radioisotope bone scan (Tc-99m) is more sensitive for detecting early osteoblastic activity but is reserved for specific indications such as suspected stress fractures, occult fractures, or suspected delayed union/non-union — not for routine early healing assessment.
Why Other Investigations Are Less Appropriate in This Context
Radioisotope Bone Scan (Tc-99m): While highly sensitive for metabolic bone activity and positive as early as 24–48 hours, it is not the investigation of choice for routine fracture healing monitoring. It is reserved for suspected non-union, occult fractures, or when plain films are inconclusive. It is less specific and involves radiation exposure.
MRI: Excellent for soft tissue and marrow edema assessment, but not the routine first-line investigation for monitoring fracture healing. Reserved for complications or soft tissue injury assessment.
CT Scan: Provides excellent bony detail and is useful for complex fractures or when plain radiographs are inconclusive, but is not required for routine early healing assessment due to higher radiation dose and cost.
Clinical Application
Plain radiography is the standard of care for:
Initial fracture assessment and classification
Monitoring fracture healing at all stages (2–3 weeks, 6 weeks, 3 months)
Assessing fracture alignment and callus formation before mobilization
Identifying complications such as malunion or non-union
Rockwood & Green's Fractures in Adults, 8th Ed., Ch. 1; Miller's Review of Orthopaedics, 7th Ed.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.