The patient is at 10 days post-fracture, which is within the inflammatory phase (0–3 weeks). The constellation of severe swelling, pain, warmth, and pain unresponsive to analgesia raises concern for compartment syndrome or excessive swelling within the rigid cast.
| Phase | Duration | Edema Status | Management Implications |
|---|---|---|---|
| Inflammatory | 0–3 weeks | Maximal swelling (peaks day 2–3) | Risk of compartment syndrome, cast splitting essential |
| Soft callus | 1–3 weeks | Swelling resolving | Cast may become loose; padding adjustment needed |
| Hard callus | 3–12 weeks | Minimal swelling | Stable immobilization |
| Remodeling | 3–12 months | Normal | Progressive loading |
Severe pain, swelling, and warmth within 10 days of fracture immobilization suggest compartment syndrome or excessive pressure necrosis. Immediate cast splitting is the standard emergency response to prevent irreversible tissue damage.
"Pain out of proportion to clinical findings" is the most sensitive early sign of compartment syndrome. In a post-fracture patient with a cast, severe pain unresponsive to analgesia should trigger immediate cast removal/splitting, not further imaging.
Do not delay treatment with imaging (MRI, CT) when compartment syndrome is suspected. Clinical examination and immediate decompression take priority. Imaging is not needed to diagnose compartment syndrome—clinical suspicion + emergency decompression is the standard.
5 P's of Compartment Syndrome — Pain (out of proportion), Pressure (tense compartment), Paresthesias, Pallor, Pulselessness (late). The first two are most reliable early signs.
Loading illustration…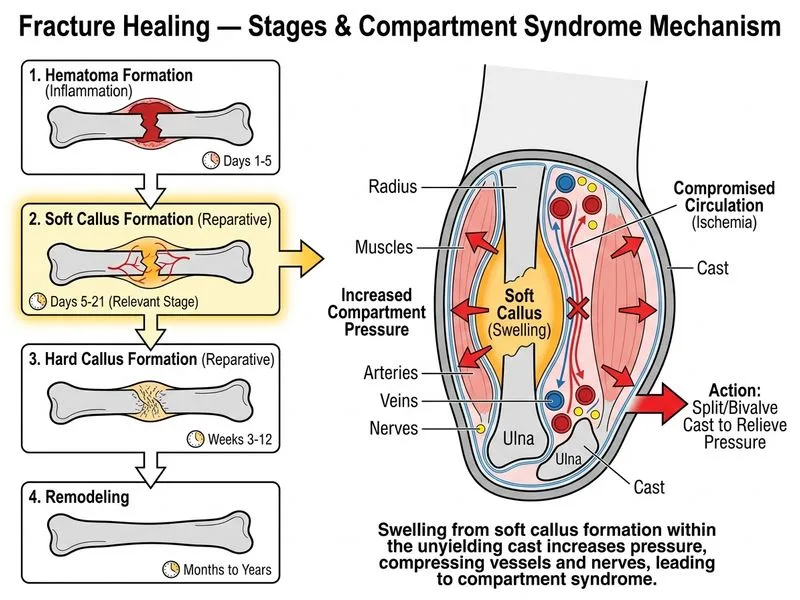
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →