## Diagnosis: Guillain-Barré Syndrome (GBS) **Key Point:** This patient presents with the classic ascending paralysis, areflexia, and albuminocytologic dissociation (elevated CSF protein with minimal cells) characteristic of GBS. The preceding diarrheal illness (likely Campylobacter jejuni) is a common trigger. ### Pathophysiology GBS is an acute autoimmune demyelinating neuropathy. Antibodies against gangliosides on myelin sheaths trigger complement-mediated demyelination and axonal damage, leading to conduction blocks and weakness. ### CSF Findings in GBS | Feature | Finding | Significance | |---------|---------|---------------| | Protein | Elevated (often >100 mg/dL) | Demyelination | | Glucose | Normal or slightly low | Reflects serum | | Cell count | <10/μL (albuminocytologic dissociation) | Minimal inflammation | | Gram stain/culture | Sterile | Rules out bacterial meningitis | ### First-Line Treatment Options **IVIg (Intravenous Immunoglobulin):** - Dose: 2 g/kg total, divided over 3–5 days (typically 0.4 g/kg/day) - Mechanism: Blocks Fc receptors, reduces antibody-mediated complement activation - Onset: 3–5 days - Advantage: Easier vascular access, fewer systemic complications **Plasma Exchange (Plasmapheresis):** - Dose: 40–50 mL/kg per exchange, 5 exchanges over 7–10 days - Mechanism: Removes circulating antibodies and complement - Onset: 2–3 days - Advantage: Faster symptom improvement in severe cases - Disadvantage: Requires central access, fluid shifts, electrolyte disturbances **High-Yield:** Both IVIg and plasma exchange are equally effective in GBS. IVIg is preferred as first-line in most centers due to ease of administration and fewer complications. Plasma exchange is reserved for severe cases, rapid progression, or IVIg failure. **Warning:** Corticosteroids (methylprednisolone) are NOT effective in GBS and may worsen outcomes — avoid. ### Supportive Care 1. **Respiratory monitoring:** FVC <15 mL/kg or NIF <-20 cm H₂O → intubation 2. **Cardiac monitoring:** Watch for dysrhythmias (autonomic dysfunction) 3. **DVT prophylaxis:** Mechanical and pharmacologic 4. **Nutritional support:** NG feeding if bulbar weakness **Clinical Pearl:** Autonomic instability (hypertension, tachycardia, arrhythmias) occurs in ~50% of GBS patients and can be life-threatening. ICU admission is warranted for severe cases. ### Why IVIg is Correct Here - Patient has confirmed GBS (clinical + NCS + CSF findings) - No contraindications to IVIg (normal renal function implied) - Easier vascular access than plasma exchange in a rural setting - Standard first-line therapy per international guidelines **Mnemonic — GBS Management: "I-PACE"** - **I** = IVIg (first-line) - **P** = Plasmapheresis (alternative) - **A** = Avoid steroids - **C** = Cardiac monitoring (autonomic) - **E** = Early respiratory support 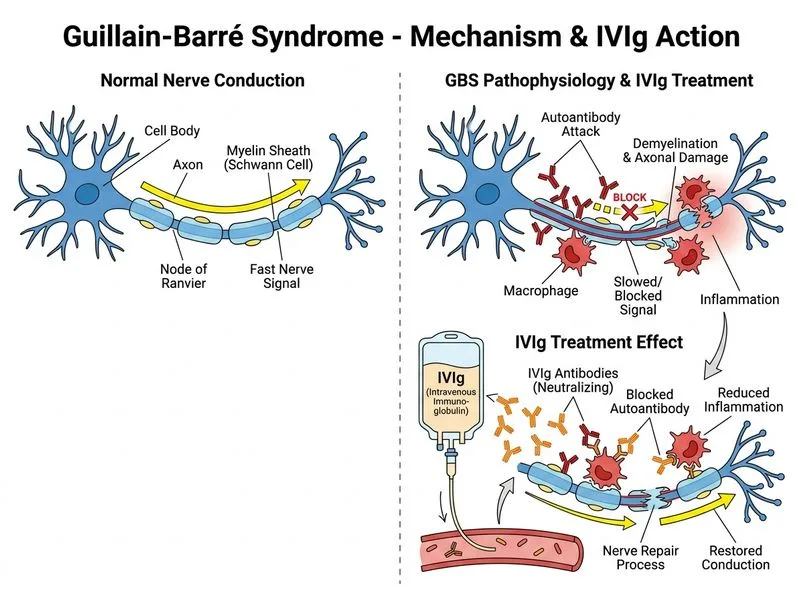
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.