Head Injury — GCS and Management MCQ — NEET PG Practice Question | NEETPGAI
Head Injury — GCS and Management
hard
scissors Surgery
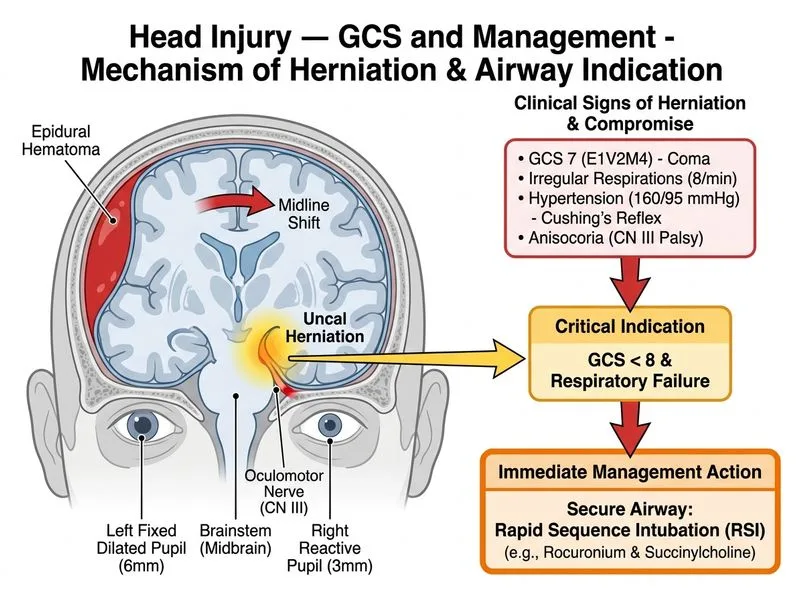
A 35-year-old woman is brought to the trauma bay after a motor vehicle collision. On primary survey, she is unconscious with a GCS of 7 (E1V2M4). Her left pupil is 6 mm and fixed; the right pupil is 3 mm and reactive. Respiratory rate is 8/min with irregular pattern. Blood pressure is 160/95 mmHg. A rapid CT head shows a large acute epidural hematoma with 8 mm midline shift and uncal herniation. What is the FIRST priority in her immediate management?
A. Immediate transfer to the operating room for epidural hematoma evacuation
B. Administer mannitol 1 g/kg IV and hyperventilate to target PaCO₂ 30–35 mmHg
C. Perform an emergency burr hole at the bedside on the side of the dilated pupil
D. Secure airway with rapid sequence intubation using rocuronium and succinylcholine
Explanation
Acute Epidural Hematoma with Herniation — Airway Priority
Key Point
A patient with GCS 7, a fixed dilated pupil (sign of uncal herniation), and respiratory depression is in acute neurological emergency. The FIRST priority is airway protection — not pharmacological management, not even neurosurgery — because without a secure airway, the patient will die from hypoxia before reaching the OR.
High-YieldNEET PG
In any head injury with GCS ≤ 8 or signs of herniation:
1.
Airway (intubate immediately)
2.
Breathing (ventilate, target normocapnia or mild hypocapnia)
3.
Circulation (maintain MAP to perfuse brain)
4.
Neurosurgery (definitive evacuation)
Triage of Interventions in Herniation
Loading diagram...
Clinical Pearl
The fixed dilated pupil (6 mm, non-reactive) on the LEFT indicates uncal herniation on that side — the ipsilateral uncus is herniating through the tentorial notch, compressing the oculomotor nerve (CN III). This is a neurosurgical emergency, but the patient cannot survive surgery without a patent airway.
Warning
Do NOT attempt burr holes at the bedside in a non-intubated patient with GCS 7 and respiratory depression. The patient will aspirate and die. Burr holes are a last resort only if the patient is in a facility with no OR and no intubation capability — exceedingly rare in modern trauma centers.
Etomidate or propofol + rocuronium is the standard RSI combination in head injury. Succinylcholine is acceptable if rocuronium is unavailable, but the transient ICP rise is a minor concern compared to airway loss.
ATLS 10th Edition, Chapter 4: Initial Assessment and Management; Neurocritical Care Society Guidelines on Traumatic Brain Injury
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.