| Feature | CT Head | MRI Brain | Skull X-ray | LP |
|---|---|---|---|---|
| Speed | <5 min | 30–45 min | <2 min | Invasive |
| Detects acute bleed | Yes (hyperdense) | Yes but slower | No | Yes but late |
| Bone fractures | Excellent | Poor | Limited | No |
| Availability | Always available | Limited in trauma | Outdated | Contraindicated |
| Radiation | Yes | No | Yes | N/A |
| Acute phase use | Gold standard | Delayed imaging | Not recommended | Contraindicated |
A GCS of 15 does not exclude intracranial injury. Up to 5–10% of patients with GCS 15 may have significant intracranial pathology on CT. Headache and neck pain in the context of trauma mandate imaging.
CT should be performed immediately in the trauma bay or resuscitation area as part of the secondary survey (ATLS protocol).
Loading illustration…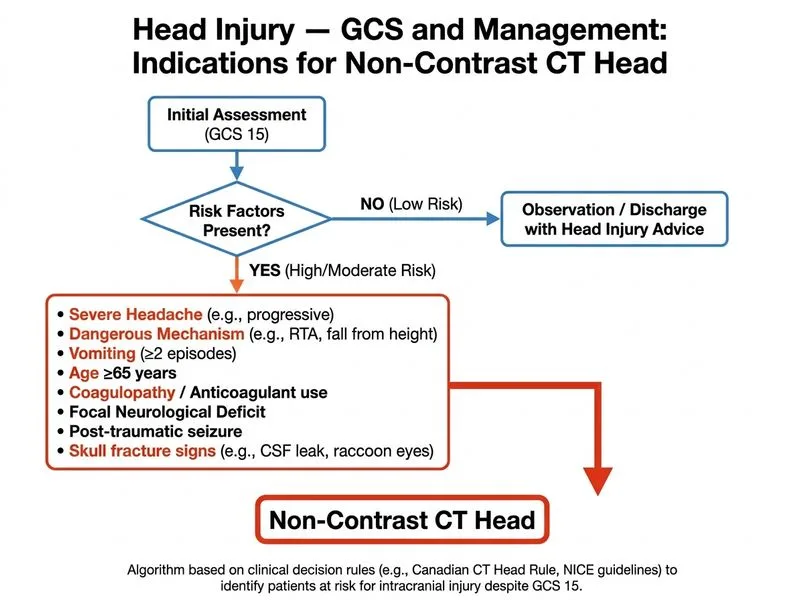
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →