A 28-year-old woman of South Indian descent presents with jaundice, dark urine, and mild abdominal pain for 3 days. She reports a similar episode 2 years ago that resolved spontaneously. On examination, she is afebrile with mild splenomegaly. Laboratory investigations show: Hemoglobin 9.2 g/dL, reticulocyte count 8.5%, indirect bilirubin 4.2 mg/dL, LDH 680 U/L, haptoglobin <10 mg/dL. Blood smear shows spherocytes and polychromasia. Osmotic fragility test is positive. Direct antiglobulin test (DAT/Coombs) is negative. What is the most likely diagnosis?
A. G6PD deficiency
B. Autoimmune hemolytic anemia
C. Sickle cell disease
D. Hereditary spherocytosis
Explanation
Clinical Diagnosis: Hereditary Spherocytosis
Key Clinical Features
Key Point
The combination of recurrent hemolytic episodes, spherocytes on blood smear, positive osmotic fragility test, and negative DAT is pathognomonic for hereditary spherocytosis (HS).
Diagnostic Reasoning
1.
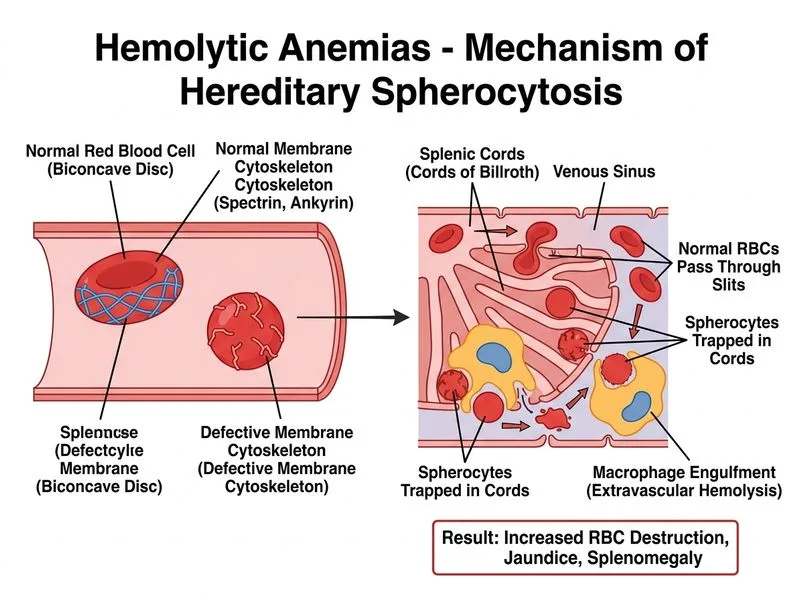
Spherocytes on blood smear — hallmark finding in HS, caused by loss of membrane surface area during repeated passage through the spleen
2.
Osmotic fragility test positive — spherocytes lyse at higher saline concentrations than normal RBCs because they have less surface area relative to volume
3.
Negative DAT — excludes autoimmune hemolytic anemia (AIHA), which would be positive
4.
Recurrent episodes — HS characteristically presents with intermittent hemolytic crises, often triggered by infections or stress
5.
South Indian ethnicity — HS has higher prevalence in certain populations; no specific ethnic predilection to G6PD in this vignette
HS results from mutations in genes encoding RBC membrane proteins (spectrin, ankyrin, band 3, protein 4.2). Loss of membrane integrity → repeated splenic passage → progressive membrane loss → spherocyte formation → splenic sequestration and hemolysis.
Why Osmotic Fragility Test Is Diagnostic
Normal RBCs can swell in hypotonic saline before lysing (they have excess membrane relative to volume). Spherocytes have already lost membrane surface area, so they lyse at higher saline concentrations (lower osmotic pressure). This test is gold standard for HS diagnosis.
Management Principles
1.
Supportive care — folic acid supplementation (increased folate demand from chronic hemolysis)
2.
Splenectomy — definitive treatment; removes primary site of RBC destruction. Should be done after age 5–6 years (post-vaccination) to reduce overwhelming post-splenectomy infection risk
3.
Vaccinations — pneumococcal, meningococcal, H. influenzae before splenectomy
Clinical Pearl
Patients with HS are at risk for aplastic crisis (transient RBC aplasia, often triggered by parvovirus B19), which presents with sudden drop in reticulocyte count and severe anemia.
Robbins 10e Ch 12
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.