Hemolytic Anemias MCQ — NEET PG Practice Question | NEETPGAI
Hemolytic Anemias
hard
microscope Pathology
A 35-year-old man of African descent presents to the emergency department with severe hemolytic anemia following a 2-week course of trimethoprim-sulfamethoxazole for a urinary tract infection. He reports dark urine and jaundice for 3 days. On examination, he is febrile (38.5°C) and has mild splenomegaly. Laboratory findings: Hemoglobin 6.8 g/dL, reticulocyte count 12%, indirect bilirubin 5.1 mg/dL, LDH 950 U/L, haptoglobin <5 mg/dL. Blood smear shows polychromasia, spherocytes, and bite cells. Direct antiglobulin test (DAT) is negative. Hemoglobin electrophoresis is normal. Which of the following is the most likely diagnosis?
A. Microangiopathic hemolytic anemia
B. G6PD deficiency with acute hemolytic crisis
C. Acute autoimmune hemolytic anemia triggered by infection
D. Hereditary spherocytosis with acute exacerbation
Explanation
Clinical Diagnosis: G6PD Deficiency with Acute Hemolytic Crisis
Key Clinical Features
Key Point
The combination of acute hemolysis triggered by a known oxidative drug (TMP-SMX), bite cells on blood smear, negative DAT, and African descent ethnicity is diagnostic of G6PD deficiency.
Diagnostic Reasoning
1.
Oxidative drug trigger — Trimethoprim-sulfamethoxazole is a classic oxidative stressor that precipitates hemolysis in G6PD-deficient patients
2.
Bite cells on blood smear — pathognomonic for G6PD deficiency; represent RBCs with Heinz bodies removed by splenic macrophages, leaving a "bite" appearance
3.
Negative DAT — excludes immune-mediated hemolysis (AIHA)
4.
African descent — G6PD deficiency is most common in African, Mediterranean, and Asian populations; ~10% of African American males are affected
5.
Acute presentation — G6PD hemolysis is episodic and triggered by oxidative stress, not chronic
6.
Normal hemoglobin electrophoresis — excludes hemoglobinopathies (sickle cell, thalassemia)
Laboratory Pattern in G6PD Deficiency
Table
Parameter
Finding
Interpretation
Hemoglobin
6.8 g/dL
Severe anemia from acute hemolysis
Reticulocyte count
12%
Markedly elevated, bone marrow response
Indirect bilirubin
5.1 mg/dL
Elevated from RBC breakdown
LDH
950 U/L
Very high, from intravascular hemolysis
Haptoglobin
<5 mg/dL
Depleted, consumed by free Hb
DAT
Negative
Excludes immune-mediated hemolysis
Blood smear
Bite cells + Heinz bodies
Pathognomonic for G6PD
Hemoglobin electrophoresis
Normal
Excludes hemoglobinopathies
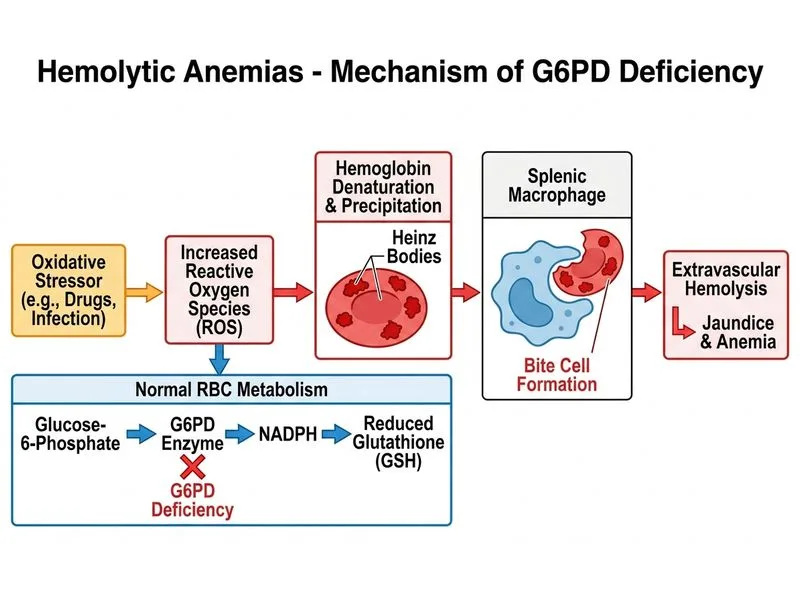
Pathophysiology of G6PD Deficiency
High-YieldNEET PG
Glucose-6-phosphate dehydrogenase is the first enzyme in the pentose phosphate pathway, essential for generating NADPH. NADPH maintains reduced glutathione (GSH), which protects RBCs from oxidative damage. G6PD deficiency → ↓NADPH → ↓GSH → oxidative stress → RBC membrane damage → hemolysis.
Heinz Bodies and Bite Cells
Mnemonic: HEINZ = Hemoglobin Enzyme Inactivation and Neoantigen Zeneration
Heinz bodies — precipitated, denatured hemoglobin visible with supravital stains (brilliant cresyl blue, new methylene blue)
Bite cells — RBCs with Heinz bodies partially removed by splenic macrophages, leaving a characteristic "bite" or indentation
Bacterial (UTI, pneumonia), viral (hepatitis A, EBV)
Foods
Fava beans (hence "favism")
Other
Acidosis, hypoxia, strenuous exercise
Why Negative DAT Rules Out AIHA
Autoimmune hemolytic anemia (AIHA) presents with positive DAT because IgG or complement is bound to RBC surface. This patient's negative DAT excludes AIHA, even though he has spherocytes (which can occur in both conditions).
Diagnosis Confirmation
Clinical Pearl
Definitive diagnosis of G6PD deficiency requires G6PD enzyme assay (quantitative or qualitative). However, during acute hemolytic crisis, reticulocytosis may falsely elevate enzyme levels (young RBCs have higher G6PD activity), so testing should be deferred 2–3 weeks after recovery.
Management
1.
Acute crisis — supportive care, transfusion if Hb <5 g/dL, IV fluids, monitor for acute kidney injury
2.
Discontinue oxidative drugs — remove TMP-SMX and any other offending agent
3.
Avoid future triggers — patient education on drugs, foods, and infections to avoid
4.
Folic acid supplementation — for chronic hemolysis (if present)
5.
No splenectomy — unlike hereditary spherocytosis, splenectomy does not help in G6PD
Warning
Do not confuse G6PD deficiency with hereditary spherocytosis. Both can present with hemolysis and spherocytes, but HS has positive osmotic fragility, HS is chronic/recurrent without clear triggers, and HS responds to splenectomy. G6PD is acute/episodic, triggered by oxidative stress, and shows bite cells (HS does not).
Robbins 10e Ch 12
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.