A 28-year-old woman from Tamil Nadu presents with jaundice, dark urine, and pallor for 3 days. On examination, she has splenomegaly and mild hepatomegaly. Hemoglobin is 7.2 g/dL, reticulocyte count 8%, indirect bilirubin 4.2 mg/dL, and haptoglobin <10 mg/dL. Peripheral blood smear shows spherocytes. Direct antiglobulin test (DAT) is strongly positive. What is the most appropriate immediate next step in management?
A. Perform osmotic fragility test and genetic counseling for hereditary spherocytosis
B. Perform bone marrow examination to rule out aplastic crisis
C. Start blood transfusion and initiate corticosteroids; arrange transfusion support as needed
D. Initiate prednisolone 1 mg/kg/day and arrange urgent splenectomy
Explanation
Clinical Diagnosis
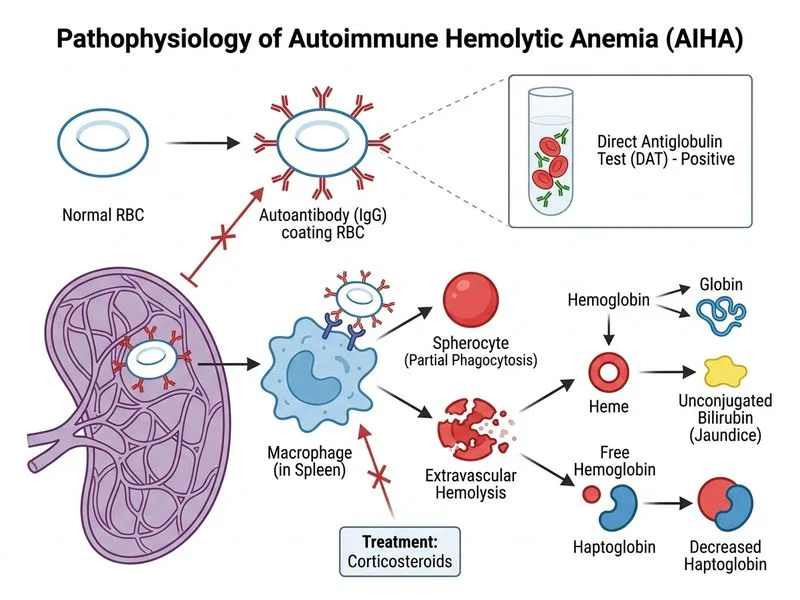
This patient has autoimmune hemolytic anemia (AIHA) with warm-antibody type, evidenced by:
Positive DAT (Coombs test) — pathognomonic for immune-mediated hemolysis
Spherocytes on smear (antibody-coated RBCs lose membrane)
Elevated indirect bilirubin and reticulocytosis
Low haptoglobin (consumed by free hemoglobin)
Splenomegaly (site of antibody-mediated RBC destruction)
Key Point
DAT positivity is the diagnostic hallmark of AIHA and distinguishes it from hereditary spherocytosis (which has negative DAT).
Management Algorithm
Loading diagram...
Why This Option Is Correct
High-YieldNEET PG
In acute AIHA with Hb 7.2 g/dL (symptomatic anemia) and positive DAT:
1.
Immediate transfusion is needed to prevent end-organ hypoxia (risk of stroke, MI, acute kidney injury)
2.
Concurrent corticosteroid initiation (prednisolone 1 mg/kg/day) suppresses antibody production and reduces hemolysis
3.
This dual approach addresses both immediate oxygen delivery and underlying immune pathology
Clinical Pearl
Transfusion in AIHA carries risk of transfused RBCs being hemolyzed, but the benefit of correcting severe anemia outweighs this risk. Use least incompatible blood if possible.
Warning
Do NOT delay transfusion waiting for splenectomy or additional testing — the patient is symptomatic with Hb <8 g/dL.
Timeline of AIHA Management
Table
Phase
Intervention
Timing
Acute (Days 1–3)
Transfusion + Corticosteroids
Immediate
Early (Weeks 1–2)
Assess response; continue steroids
Ongoing
Maintenance (Weeks 2–12)
Taper prednisolone if responding
Gradual
Refractory (>2 weeks)
Add azathioprine, rituximab, or splenectomy
If needed
Mnemonic: AIHA Management = TCS (Transfuse, Corticosteroids, Splenectomy if refractory)
Why Splenectomy Is NOT First-Line Here
Splenectomy is reserved for:
Corticosteroid-dependent or refractory cases (after 2–4 weeks of steroid trial)
Patients requiring unacceptable steroid doses to maintain remission
NOT as immediate therapy in acute presentation
Urgent splenectomy in option 1 is premature and inappropriate.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.