This patient has glucose-6-phosphate dehydrogenase (G6PD) deficiency with acute hemolytic crisis triggered by an oxidative stressor (trimethoprim-sulfamethoxazole).
| Step | Intervention | Rationale |
|---|---|---|
| Immediate | Discontinue offending drug | Removes oxidative stress; allows RBC recovery |
| Immediate | IV hydration (0.9% saline) | Prevents acute kidney injury from hemoglobinuria |
| Monitoring | Urinalysis, urine output, serum creatinine | Detect hemoglobinuria and renal dysfunction |
| Supportive | Transfusion only if Hb <7 or symptomatic | Avoid unnecessary transfusion; crisis is self-limited |
| Prevention | Folic acid 5 mg daily during recovery | Supports RBC regeneration (given AFTER acute phase) |
| Education | Avoid triggers: sulfonamides, NSAIDs, fava beans, infections | Prevent future crises |
Mnemonic: G6PD Crisis Management = DHUM (Discontinue drug, Hydrate, Urine monitor, Manage supportively)
The four pillars of immediate management are:
Loading illustration…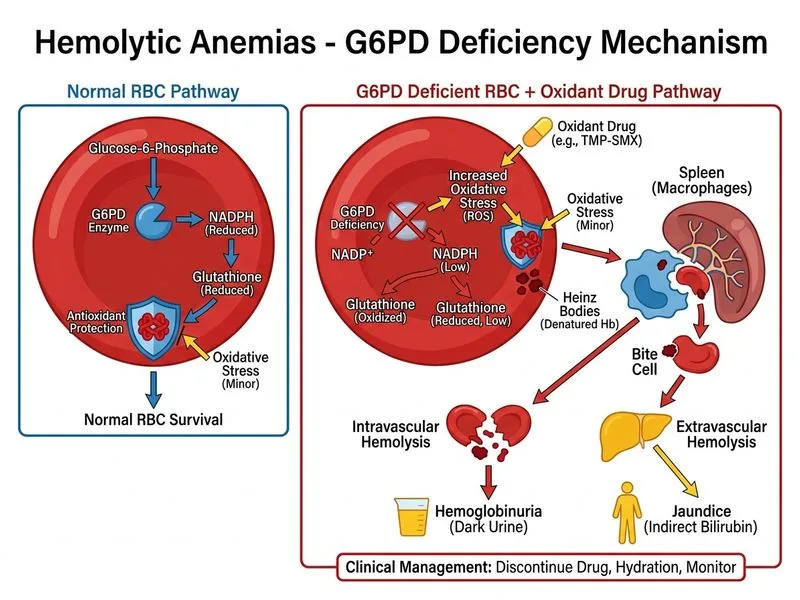
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →