## Clinical Diagnosis: AIHA Superimposed on Hereditary Spherocytosis ### Key Clinical Features **Key Point:** A patient with chronic hereditary spherocytosis (baseline Hb 8–9 g/dL, spherocytes on smear) now presenting with acute hemolysis, positive DAT, and clinical signs of immune-mediated hemolysis (fever, recent infection trigger) indicates autoimmune hemolytic anemia (AIHA) superimposed on the underlying hereditary condition. ### Differential Diagnosis Table | Feature | AIHA + HS | Acute HS Crisis | Parvovirus B19 | TTP | |---------|-----------|-----------------|----------------|-----| | **Baseline Hb** | Chronically low (8–9) | Chronically low (8–9) | Normal or mild ↓ | Normal | | **DAT** | **Positive** | Negative | Negative | Negative | | **Spherocytes** | Yes (HS) | Yes (HS) | No | Schistocytes | | **Reticulocyte response** | Brisk (18%) | Brisk but may be blunted | **Absent/very low** | Variable | | **Fever** | **Yes** (immune trigger) | No | Yes (viral) | Yes (TTP) | | **Trigger** | Infection, autoimmune | Osmotic stress, infection | Viral infection | Microangiopathy | | **Platelets** | Normal | Normal | Normal | **Low** | | **Neurological signs** | No | No | No | **Yes** | ### Pathophysiology of AIHA Superimposed on HS 1. **Baseline hereditary spherocytosis:** RBCs have abnormal membrane proteins (spectrin, ankyrin, band 3), leading to chronic compensated hemolysis 2. **Immune trigger (infection):** Recent URTI activates T-cell and B-cell responses, producing anti-RBC IgG antibodies 3. **Complement activation:** IgG and complement bind to RBC surface, detected by positive DAT 4. **Accelerated hemolysis:** Splenic macrophages recognize antibody-coated RBCs and destroy them via antibody-dependent cellular cytotoxicity (ADCC) 5. **Clinical result:** Acute drop in Hb from baseline, severe jaundice, dark urine (hemoglobinuria possible if severe) **High-Yield:** A positive DAT in a patient with known spherocytosis is the key finding distinguishing AIHA superimposed on HS from a simple acute crisis of HS alone. ### Why This Is Not the Other Diagnoses #### Parvovirus B19 Infection - Causes **aplastic crisis** (not hemolytic crisis) in HS patients - Characterized by **absent or very low reticulocyte count** (bone marrow suppression) - This patient has a brisk reticulocyte response (18%), ruling out aplastic crisis - DAT is negative in parvovirus B19 #### Acute HS Crisis (Splenic Sequestration) - Occurs without immune trigger; DAT is **negative** - Reticulocyte response is present but not accompanied by positive DAT - Fever is absent unless secondary infection - No evidence of IgG/complement coating on RBCs #### Thrombotic Thrombocytopenic Purpura (TTP) - Would present with **thrombocytopenia** (not mentioned; platelets assumed normal) - Schistocytes on smear (not spherocytes) - Neurological and renal involvement (not described) - DAT is negative ### Diagnostic Approach ```mermaid flowchart TD A[Chronic hemolytic anemia with spherocytes]:::outcome --> B{DAT positive?}:::decision B -->|Yes| C[AIHA superimposed on HS]:::outcome B -->|No| D{Reticulocyte count?}:::decision D -->|Brisk| E[Acute HS crisis]:::outcome D -->|Absent/low| F[Aplastic crisis - consider parvovirus B19]:::outcome C --> G[Treat with corticosteroids + supportive care]:::action E --> H[Supportive care, treat trigger]:::action F --> I[Transfusion support, monitor marrow recovery]:::action ``` ### Management of AIHA Superimposed on HS 1. **Immediate:** - Transfusion if Hb <5 g/dL or symptomatic (use blood bank protocol for warm AIHA) - Treat underlying infection (antibiotics for URTI) 2. **Immunosuppression:** - **Corticosteroids** (prednisolone 1 mg/kg/day) — first-line - Taper over 2–3 months based on response - Response rate ~80% in warm AIHA 3. **Splenectomy:** - Consider if steroid-dependent or steroid-resistant - Effective in ~60–70% of HS + AIHA cases - Reduces both HS hemolysis and antibody production 4. **Second-line agents (if steroid failure):** - Rituximab (anti-CD20 monoclonal antibody) - Azathioprine or mycophenolate mofetil - Intravenous immunoglobulin (IVIG) — temporary benefit **Clinical Pearl:** Patients with hereditary spherocytosis are at risk for AIHA, especially after infections. The combination of chronic baseline hemolysis and acute immune-mediated destruction can cause life-threatening anemia requiring urgent intervention. **Mnemonic:** **DAIS** for AIHA diagnosis — **D**AT positive, **A**ntibody-coated RBCs, **I**mmune trigger (infection, drugs, autoimmune disease), **S**plenomegaly and hemolysis. [cite:Robbins 10e Ch 12; Harrison 21e Ch 139] 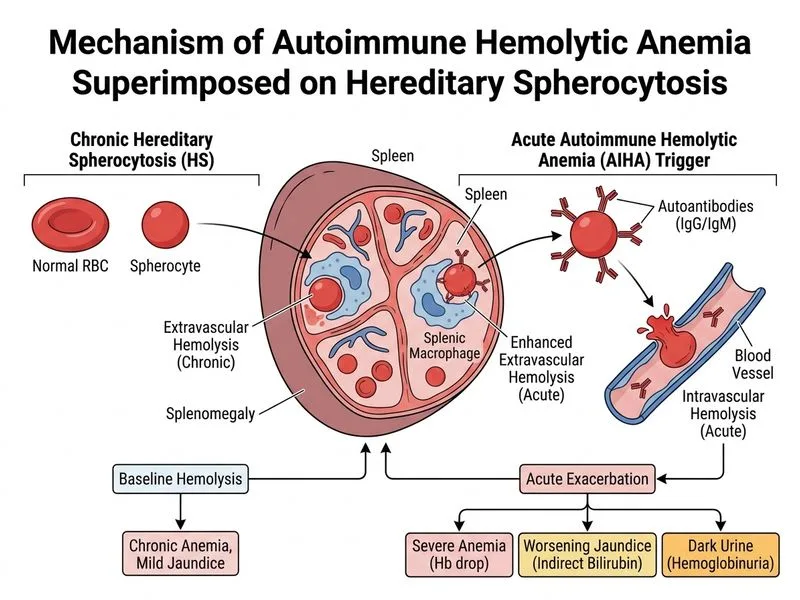
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.