For nodules in cirrhotic livers:
| Nodule Size | Imaging Criteria for HCC Diagnosis |
|---|---|
| >2 cm | One imaging modality (CT/MRI/US) with arterial phase hyperenhancement (APHE) + washout |
| 1–2 cm | Two imaging modalities showing APHE + washout, OR one imaging modality + AFP >400 ng/mL |
| <1 cm | Surveillance; biopsy if high suspicion |
Chronic HBV infection → chronic inflammation → cirrhosis → dysplastic nodules → HCC. HBV integration into hepatocyte genome and HBx protein expression drive malignant transformation.
Arterial phase hyperenhancement (APHE) followed by venous/delayed phase washout is the pathognomonic imaging signature of HCC — reflects tumor's arterial blood supply (from hepatic artery) rather than portal venous supply of normal liver parenchyma.
Loading illustration…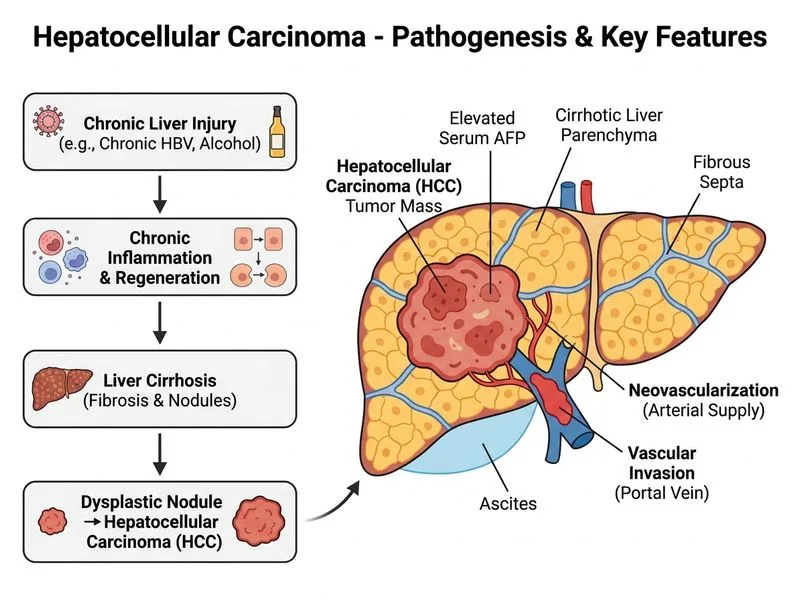
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →