In cirrhotic livers:
| Nodule Size | Diagnostic Criteria |
|---|---|
| >20 mm | APHE + washout on one imaging modality (CT/MRI) |
| 10–20 mm | APHE + washout on both CT AND MRI, OR biopsy |
| <10 mm | Follow-up imaging (too small for reliable diagnosis) |
Robbins 10e Ch 20
Loading illustration…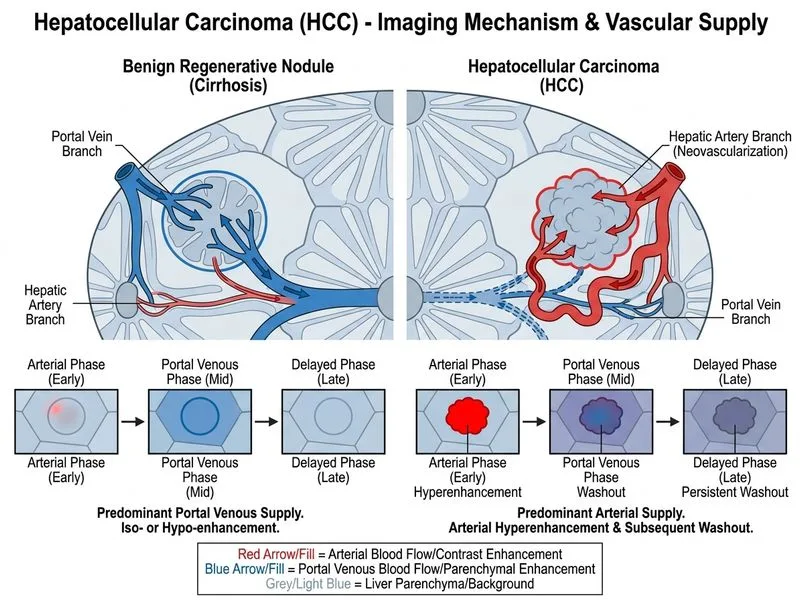
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →