Hepatocellular Carcinoma MCQ — NEET PG Practice Question | NEETPGAI
Hepatocellular Carcinoma
hard
microscope Pathology
A 62-year-old Indian man with HBsAg-positive cirrhosis presents with a 3 cm liver nodule. Biopsy shows well-differentiated HCC. Which histological feature best distinguishes well-differentiated HCC from benign cirrhotic nodules (adenomatous hyperplasia)?
A. Presence of fibrous capsule surrounding the nodule
B. Fatty change and lipid accumulation in tumor cells
C. Increased mitotic activity and marked nuclear pleomorphism
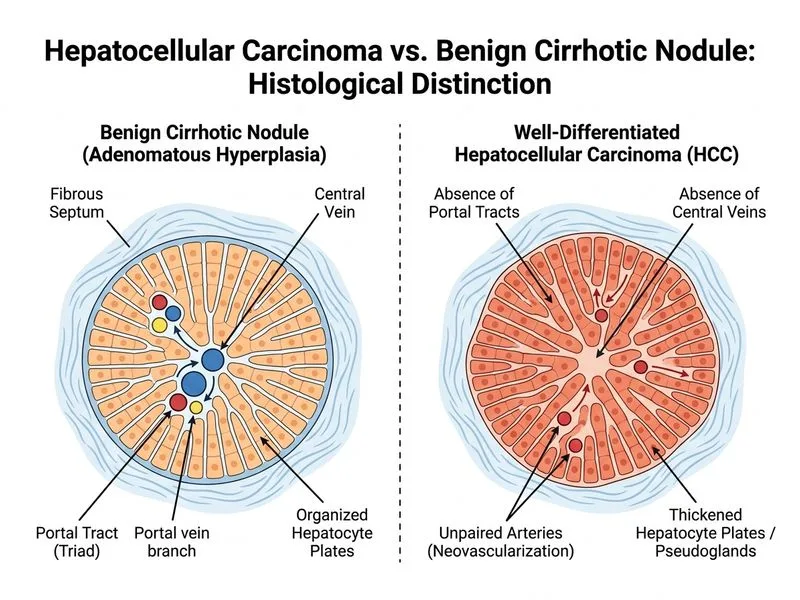
D. Absence of portal tracts and central veins within the nodule
Explanation
Histopathology: HCC vs. Benign Cirrhotic Nodules
The Diagnostic Dilemma: Well-Differentiated HCC
Key Point
Well-differentiated HCC is histologically challenging to distinguish from adenomatous hyperplasia (benign). The single most reliable discriminator is the absence of portal tracts and central veins within the nodule — a feature that reflects loss of the normal acinar architecture.
Architectural Features
Table
Feature
Well-Differentiated HCC
Adenomatous Hyperplasia
Regenerative Nodule
Portal tracts
Absent or markedly reduced
Present (though may be compressed)
Present
Central veins
Absent or displaced
Present
Present
Fibrous capsule
May be present (not diagnostic)
Absent
Absent
Trabecular pattern
Thickened (>1 cell thick)
Normal (1 cell thick)
Normal
Nuclear atypia
Mild to moderate
Minimal
Minimal
Mitotic rate
Increased
Normal
Normal
High-YieldNEET PG
The absence of portal tracts and central veins is the most specific architectural feature because it indicates loss of the normal lobular framework — a hallmark of HCC even when cytological atypia is subtle.
Why Cytological Features Are Unreliable in Well-Differentiated HCC
1.
Increased mitotic activity — can be seen in regenerating cirrhotic nodules, especially in active hepatitis
2.
Nuclear pleomorphism — may be absent in well-differentiated HCC and present in benign nodules with inflammation
3.
These features overlap between HCC and reactive/regenerative changes
Clinical Pearl
When a small HCC is well-differentiated and cytologically subtle, immunohistochemistry (GPC3, HSP70, glutamine synthetase) can support the diagnosis, but architectural loss (absent portal tracts) remains the gold standard.
Fibrous Capsule: A Trap
Warning
A fibrous capsule is present in ~30% of HCCs and is a sign of compression by the tumor, not a feature that distinguishes HCC from benign nodules. Benign nodules do NOT have capsules, but the presence of a capsule in HCC does not help differentiate it from adenomatous hyperplasia.
Fatty Change: Non-Specific
Fatty change (steatosis) can occur in both HCC and benign nodules, especially in metabolic syndrome or NAFLD-related cirrhosis. It is not discriminatory.
Robbins 10e Ch 20
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.