| Dermatome Region | Frequency | Clinical Notes |
|---|---|---|
| Thoracic (T1–L2) | 50–60% | Most common; typically unilateral, follows rib distribution |
| Cervical (C2–C4) | 10–20% | Second most common |
| Lumbar/Sacral (L1–S5) | 10–15% | Lower frequency |
| Ophthalmic (V1) | 10–15% | Risk of ocular complications; requires urgent ophthalmology referral |
| Other cranial nerves | 5–10% | Ramsay Hunt syndrome (CN VII), CN V2/V3 |
Park 26e Ch 8
Loading illustration…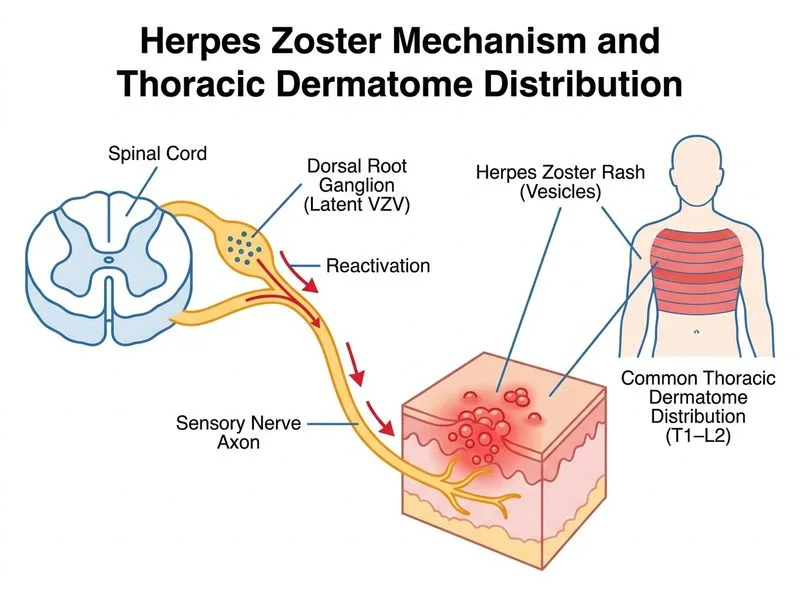
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →