Herpes Simplex and Zoster — Skin MCQ — NEET PG Practice Question | NEETPGAI
Herpes Simplex and Zoster — Skin
medium
hand Dermatology
A 34-year-old woman presents with a 3-day history of painful vesicular eruption in a dermatomal distribution on her left chest wall. She reports severe burning pain that preceded the rash by 2 days. On examination, grouped vesicles on an erythematous base are seen in the T4–T6 dermatome. She is afebrile and systemically well. She has no prior history of chickenpox but received varicella vaccine 10 years ago. What is the most likely diagnosis?
A. Herpes simplex virus type 1 with dermatomal spread
B. Contact dermatitis with secondary bacterial infection
C. Herpes zoster (shingles)
D. Disseminated varicella-zoster virus in an immunocompromised host
Explanation
Clinical Diagnosis: Herpes Zoster
Key Distinguishing Features
Key Point
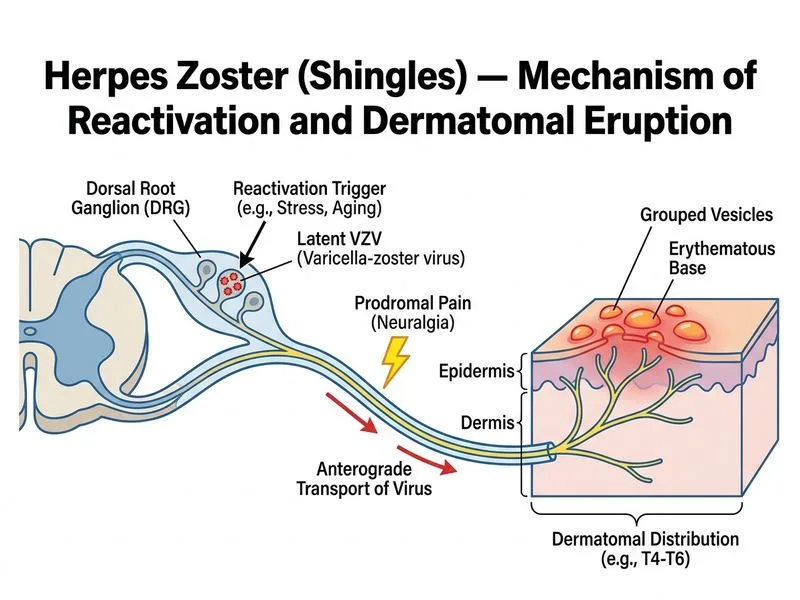
Herpes zoster (shingles) is characterized by a unilateral, dermatomal distribution of painful vesicles, typically preceded by 2–3 days of prodromal pain (neuropathic burning or itch).
Pathophysiology
Herpes zoster results from reactivation of latent varicella-zoster virus (VZV) in dorsal root ganglia. The virus travels along a single sensory nerve, producing a dermatomal rash. Vaccination does not prevent reactivation but may reduce severity and post-herpetic neuralgia risk.
Clinical Features Supporting This Case
Table
Feature
Finding in This Case
Significance
Distribution
Unilateral, T4–T6 dermatome
Pathognomonic for zoster
Prodrome
2 days of burning pain before rash
Classic neuropathic pain precedes lesions
Lesion morphology
Grouped vesicles on erythematous base
Identical to primary VZV (varicella)
Systemic signs
Afebrile, systemically well
Typical for immunocompetent host
Age
34 years
Can occur at any age; risk increases >50 years
Diagnostic Approach
High-YieldNEET PG
Clinical diagnosis is usually sufficient. If confirmation needed:
Tzanck smear: Multinucleated giant cells (not specific for VZV vs. HSV)
PCR or viral culture: Gold standard; differentiates VZV from HSV
Direct fluorescent antibody (DFA): Rapid, specific for VZV
Management Principles
1.
Antivirals (within 72 hours of rash onset for maximal benefit):
Acyclovir 800 mg 5× daily × 7–10 days, OR
Valacyclovir 1000 mg 3× daily × 7 days (preferred; better bioavailability), OR
Famciclovir 500 mg 3× daily × 7 days
2.
Analgesia: NSAIDs, pregabalin, or gabapentin for neuropathic pain
3.
Post-herpetic neuralgia (PHN) prevention: Antivirals reduce PHN risk by ~50% if started early
Clinical Pearl
Dermatomal distribution is the single most reliable clinical clue distinguishing zoster from HSV-1 (which is typically non-dermatomal, recurrent at same site, and preceded by prodrome at that site).
Mnemonic: ZOSTER Features
Zoster = reactivation (vs. primary varicella)
One dermatome (unilateral)
Severe pain (neuropathic, often precedes rash)
Treatment window: <72 hours for antivirals
Eruption: grouped vesicles on erythema
Risk: age >50, immunosuppression, malignancy
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.