| Criterion | Rationale |
|---|---|
| CD4 <100 | Severe immunosuppression increases risk of disseminated VZV, post-herpetic neuralgia, and ocular complications |
| Corneal involvement | Requires high CNS/aqueous humor penetration; IV acyclovir achieves superior levels vs. oral formulations |
| V1 distribution | Ophthalmic zoster carries 50–70% risk of ocular sequelae if not aggressively treated |
| Systemic risk | CD4 <100 confers risk of VZV vasculopathy (stroke) and disseminated disease |
Loading illustration…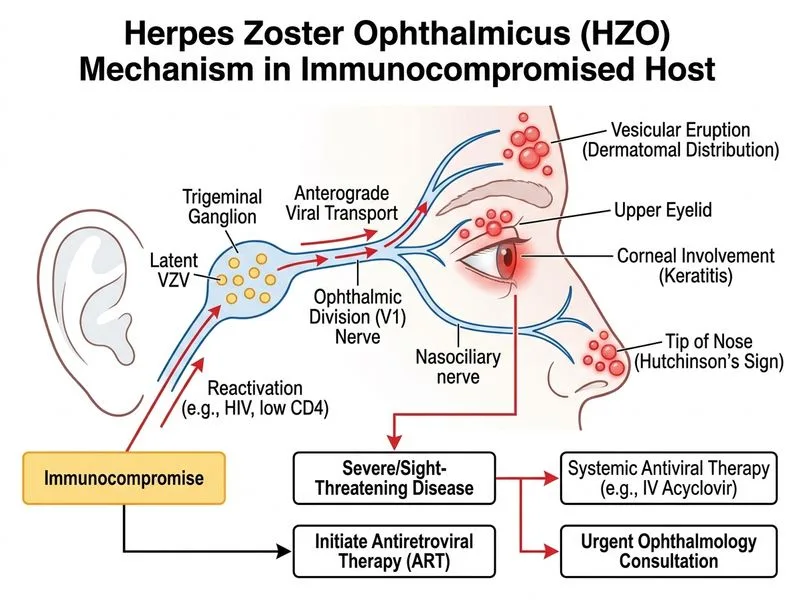
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →