A 32-year-old woman presents with a 3-day history of painful vesicular rash in a dermatomal distribution on the left thorax. She reports severe pain and burning sensation. On examination, grouped vesicles on an erythematous base are seen in the T5–T6 dermatome. She is otherwise healthy with no immunosuppression. What is the most appropriate immediate management?
A. Perform PCR of vesicular fluid to confirm diagnosis before starting antiviral therapy
B. Refer to neurology for assessment of postherpetic neuralgia risk
C. Start oral acyclovir 800 mg five times daily for 7–10 days
D. Apply topical acyclovir cream and observe for spontaneous resolution
Explanation
Clinical Context
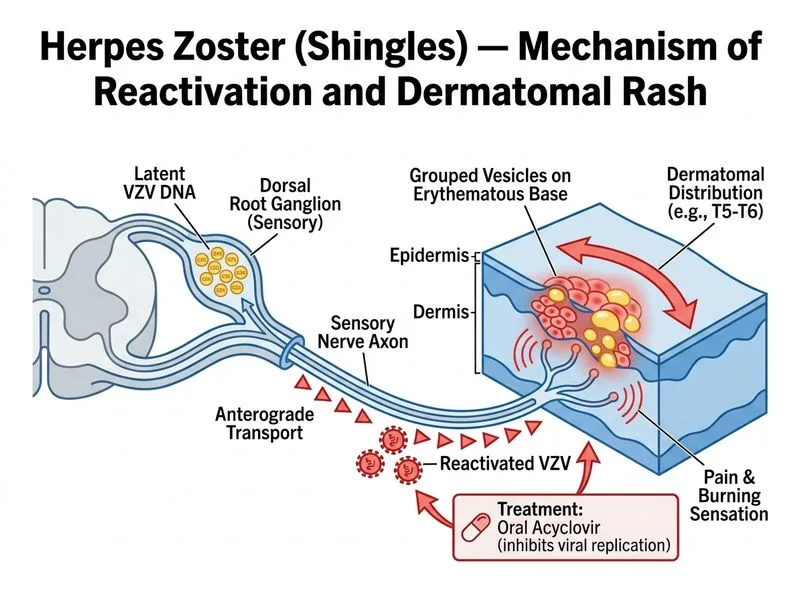
This patient presents with classic herpes zoster (shingles) — dermatomal vesicular rash with severe pain in an immunocompetent adult. The diagnosis is clinical; no confirmatory testing is required before initiating antiviral therapy.
Management Principles for Acute Zoster
Key Point
Antiviral therapy must be started within 72 hours of rash onset to be most effective in reducing pain, duration of viral shedding, and risk of postherpetic neuralgia (PHN).
High-YieldNEET PG
In immunocompetent adults with dermatomal zoster:
First-line agent: Oral acyclovir 800 mg five times daily for 7–10 days
Alternative: Valacyclovir 1000 mg three times daily or famciclovir 500 mg three times daily (higher bioavailability, but acyclovir is standard in India)
Timing: Initiate within 72 hours of rash onset for maximum benefit
Clinical Pearl
Early antiviral therapy reduces acute pain duration by ~1 week and decreases the incidence of PHN (especially in patients >50 years). Even though this patient is 32, prompt treatment is still indicated.
Why Oral Acyclovir 800 mg 5× Daily is Correct
1.
Proven efficacy: Reduces viral shedding, shortens lesion healing time, and decreases PHN risk when started early
2.
Timing: Patient is within 72-hour window — the critical period for antiviral benefit
3.
Immunocompetent status: Oral therapy is sufficient; IV acyclovir is reserved for disseminated disease or immunocompromised hosts
4.
Standard dosing: 800 mg five times daily (not 400 mg) is the recommended dose for zoster
Adjunctive Management
Table
Intervention
Indication
Analgesics (paracetamol, NSAIDs)
Pain control during acute phase
Tricyclic antidepressants (amitriptyline)
Prevention/management of PHN (start if pain persists >1 month)
Topical lidocaine patches
Localized pain relief after crusting
Corticosteroids
Controversial; may reduce PHN in patients >50 years (adjunctive only)
Tip
Do not delay antiviral therapy while awaiting confirmatory tests — clinical diagnosis is sufficient, and early treatment improves outcomes.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.