## Iatrogenic CBD Perforation During Cholecystectomy **Key Point:** Management of CBD perforation depends on timing of recognition (intraoperative vs. postoperative), size, and location. **Correct Answer: Primary Closure with T-tube Stent** ### Rationale for Intraoperative Recognition: - **Timing advantage:** Recognized intraoperatively → allows immediate definitive repair - **Small perforation (<3 mm):** Primary closure is appropriate - **Technique:** 5-0 absorbable suture (Vicryl) with interrupted stitches - **T-tube stent:** Essential for small perforations to: - Protect the repair site - Prevent stricture formation - Allow controlled drainage - Facilitate future cholangiography - **Success rate:** >95% with primary closure + T-tube for small perforations ### High-Yield Mnemonic: **SCOT** - **S**mall perforation (<3 mm) → Primary closure + T-tube - **C**omplete transection → Hepaticojejunostomy - **O**pen surgery conversion (often needed) - **T**-tube for protection ### Clinical Pearl: Large perforations (>3 mm) or complete transection require hepaticojejunostomy (Roux-en-Y), not simple closure. ### Table: CBD Perforation Management | Perforation Size | Timing | Management | |---|---|---| | <3 mm | Intraoperative | Primary closure + T-tube | | 3–5 mm | Intraoperative | Primary closure ± T-tube or HJ | | >5 mm or transection | Intraoperative | Hepaticojejunostomy (Roux-en-Y) | | Any size | Postoperative | ERCP ± stent ± PTC drain | 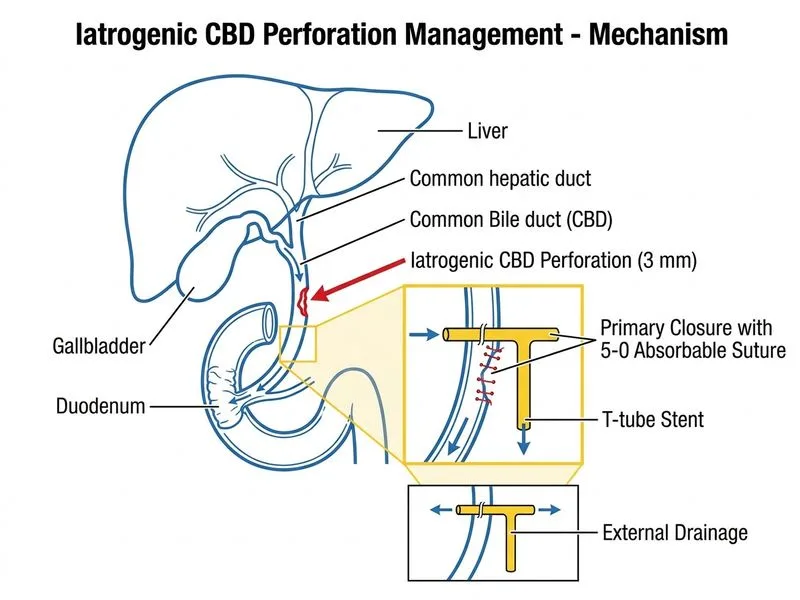
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.