Impetigo and Staphylococcal Skin Infections MCQ — NEET PG Practice Question | NEETPGAI
Impetigo and Staphylococcal Skin Infections
medium
hand Dermatology
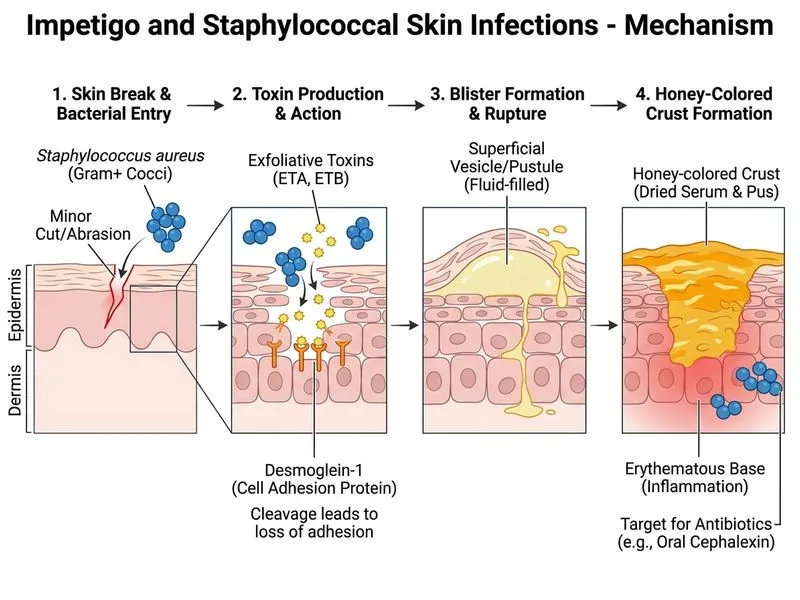
A 4-year-old boy from rural Maharashtra presents with his mother to the outpatient clinic with multiple fluid-filled blisters on his left forearm and hand that appeared 3 days ago. The lesions are preceded by a small cut sustained while playing. On examination, there are honey-crusted erosions overlying erythematous patches. The child is afebrile. A Gram stain of the blister fluid shows Gram-positive cocci in clusters. What is the most likely causative organism and the recommended first-line treatment?
A. Streptococcus pyogenes; intramuscular penicillin G
B. Corynebacterium diphtheriae; oral erythromycin
C. Staphylococcus epidermidis; topical mupirocin
D. Staphylococcus aureus; oral cephalexin
Explanation
Diagnosis: Non-bullous Impetigo
Clinical Presentation
Key Point
The honey-crusted erosions on an erythematous base are pathognomonic for non-bullous impetigo, which accounts for ~70% of impetigo cases in India.
The clinical triad:
1.
Preceding minor trauma (cut while playing)
2.
Rapid onset (3 days)
3.
Honey-coloured crusts on erythematous base
Microbiology
High-YieldNEET PG
Gram-positive cocci in clusters = Staphylococcus aureus. This is now the most common cause of impetigo globally, including in India, displacing Streptococcus pyogenes.
Table
Feature
S. aureus
S. pyogenes
Gram stain
Cocci in clusters
Cocci in chains
Impetigo prevalence
~70% (current)
~30%
Bullous impetigo
Common (exfoliative toxin)
Rare
Non-bullous impetigo
Common
Less common
Treatment Algorithm
Loading diagram...
Key Point
Oral cephalexin (a first-generation cephalosporin) is the preferred first-line oral agent for impetigo because it:
Covers both S. aureus and S. pyogenes
Has excellent skin penetration
Is well-tolerated in children
Is cost-effective in India
Clinical Pearl
Although this child has localized lesions (one forearm), the presence of multiple lesions and the need for systemic coverage of both organisms makes oral cephalexin appropriate. Topical mupirocin alone may be considered for <5 lesions in a compliant family.
Why Not Penicillin G?
Warning
Intramuscular penicillin G is NOT first-line for impetigo because:
Many S. aureus strains are penicillin-resistant (β-lactamase producers)
Oral agents are preferred for non-severe impetigo
IM injection is unnecessary for localized skin infection
Penicillin G remains useful for invasive streptococcal infections (cellulitis, erysipelas) but not for impetigo.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.