| Presentation | First-line Treatment | Rationale |
|---|---|---|
| Localized (< 5 lesions or < 2% BSA) | Topical mupirocin 2% TDS | High efficacy, minimal systemic absorption, prevents spread |
| Localized with poor hygiene | Topical mupirocin + oral antibiotic | Dual approach to reduce carriage |
| Generalized (> 5 lesions or > 2% BSA) | Oral β-lactamase-resistant penicillin or cephalosporin | Systemic coverage for Staph aureus |
| Bullous impetigo | Oral antibiotic ± topical | Deeper dermal involvement |
Mechanism: Mupirocin inhibits bacterial isoleucyl-tRNA synthetase, halting protein synthesis.
Loading illustration…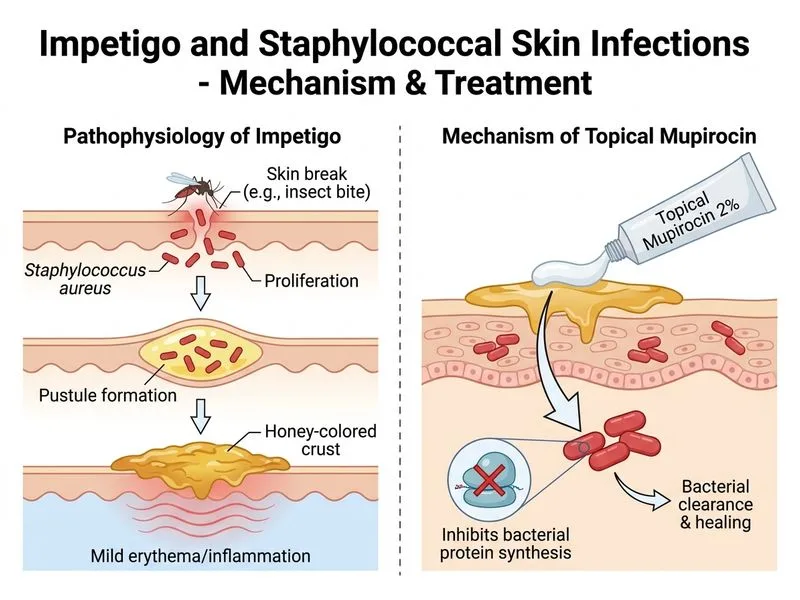
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →