Impetigo and Staphylococcal Skin Infections MCQ — NEET PG Practice Question | NEETPGAI
Impetigo and Staphylococcal Skin Infections
medium
hand Dermatology
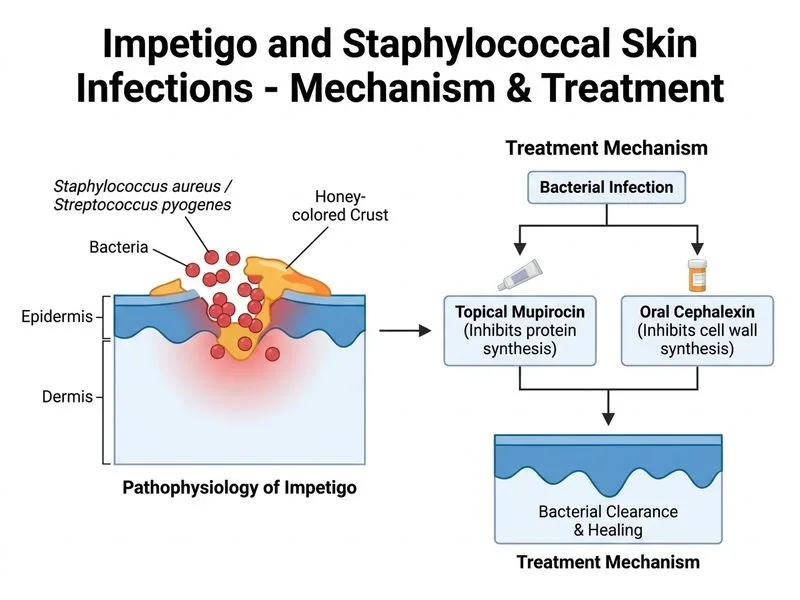
A 6-year-old girl presents with multiple honey-crusted lesions scattered over both arms, legs, and trunk for 10 days. Mother reports poor hygiene and the child attends a crowded school. Lesions are non-bullous, painless, and some show early signs of crusting. Temperature is 37.2°C. On examination, there is mild cervical lymphadenopathy but no cellulitis. What is the most appropriate next step in management?
A. Oral cephalexin 500 mg QID for 7 days plus topical mupirocin
B. Topical mupirocin 2% to all lesions TDS for 7 days
C. Oral cloxacillin 500 mg QID for 7 days alone
D. Refer for hospitalization and IV antibiotics
Explanation
Clinical Assessment
Key Point
This patient has non-bullous impetigo with lesions on multiple body sites. However, the clinical picture — no fever (37.2°C is normal), no cellulitis, only mild cervical lymphadenopathy (reactive, not suppurative), and no systemic toxicity — does not mandate oral antibiotics. Current evidence-based guidelines (AAP, IDSA, British Association of Dermatology) recommend topical mupirocin 2% as first-line therapy for non-bullous impetigo regardless of the number of lesions, unless there is systemic involvement or treatment failure.
Impetigo Management Algorithm
code
Non-bullous impetigo
|
├── No systemic signs (no fever, no cellulitis, no toxicity)
| → Topical mupirocin 2% TDS × 5–7 days ✔
|
├── Systemic signs / extensive involvement / immunocompromised
| → Oral antibiotic (cephalexin or cloxacillin)
|
└── Hospitalization / IV antibiotics
→ Only for sepsis, SSSS, or severe cellulitis
Why Topical Mupirocin Alone is Correct
High-YieldNEET PG
The IDSA 2014 guidelines and multiple RCTs (Koning et al., Cochrane 2012) demonstrate:
Topical mupirocin is equivalent to oral antibiotics for non-bullous impetigo without systemic signs.
Adding oral antibiotics to topical therapy does not improve cure rates in uncomplicated cases and increases antibiotic resistance risk.
The presence of lesions on multiple body sites alone does NOT constitute an indication for oral antibiotics in the absence of systemic toxicity, cellulitis, or immunocompromise.
Clinical Pearl
Mild cervical lymphadenopathy is a reactive finding commonly seen with impetigo and does NOT indicate systemic infection requiring oral antibiotics. It resolves with successful topical treatment.
Why Other Options Are Incorrect
Table
Option
Reason Incorrect
B) Oral cephalexin + topical mupirocin
Combination not superior to topical alone in uncomplicated non-bullous impetigo; over-treatment
C) Oral cloxacillin alone
Topical therapy preferred; monotherapy without topical mupirocin is suboptimal
D) IV antibiotics / hospitalization
No systemic toxicity, no SSSS, no sepsis — hospitalization not indicated
Topical Mupirocin Regimen
Mupirocin 2% ointment applied TDS (three times daily) to all lesions
Duration: 5–7 days
Gently remove crusts with warm water before application to improve penetration
Advise hand hygiene and avoid sharing towels/clothing to prevent school transmission
Reference: IDSA Clinical Practice Guidelines for Skin and Soft Tissue Infections (Stevens et al., CID 2014); Fitzpatrick's Dermatology, 9th edition.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.