A 28-year-old woman from Delhi presents with a 6-month history of bloody diarrhea, abdominal cramping, and weight loss of 4 kg. She reports 6–8 bowel movements daily with blood and mucus. On examination, she is afebrile, abdomen is soft with mild left lower quadrant tenderness. Laboratory findings: hemoglobin 9.2 g/dL, ESR 68 mm/hr, CRP 12 mg/dL, fecal calprotectin 420 μg/g (normal <50). Colonoscopy reveals continuous mucosal inflammation with friability and loss of haustra, limited to the colon. Histopathology shows crypt distortion, increased chronic inflammation in the lamina propria, and absence of granulomas. What is the most likely diagnosis?
A. Irritable bowel syndrome
B. Infectious colitis due to Entamoeba histolytica
C. Ulcerative colitis
D. Crohn disease
Explanation
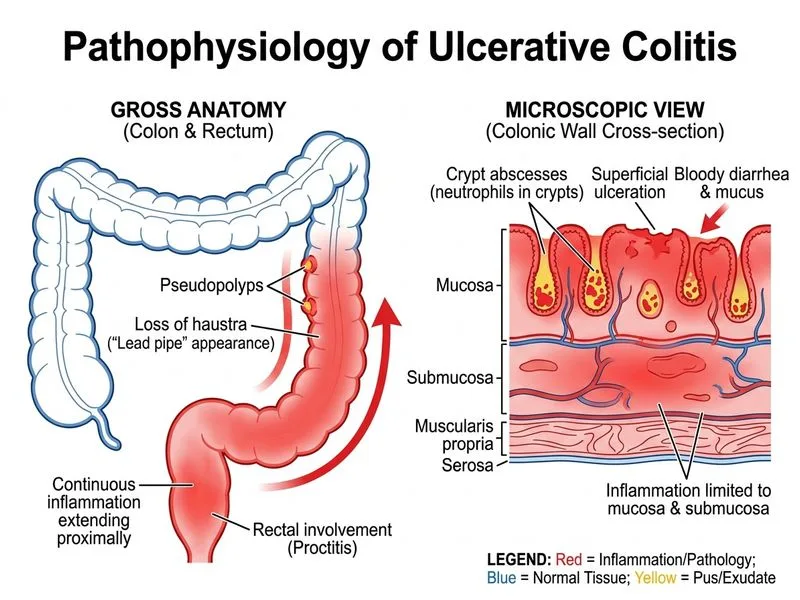
Diagnosis: Ulcerative Colitis
Clinical Presentation
The patient presents with the classic triad of ulcerative colitis:
Bloody diarrhea with mucus (hallmark feature)
Continuous colonic involvement without skip lesions
Systemic inflammation (elevated ESR, CRP, high fecal calprotectin)
Key Pathological Features
Table
Feature
Ulcerative Colitis
Crohn Disease
Distribution
Continuous, colon only
Skip lesions, any part of GI tract
Depth of inflammation
Mucosa and submucosa
Transmural (full thickness)
Crypt distortion
Present
Present
Granulomas
Absent
Present in 30–50%
Fissuring ulcers
Rare
Common
Haustra
Loss of haustra (lead pipe appearance)
Preserved initially
Key Point
The absence of granulomas on histology, continuous mucosal inflammation limited to the colon, and loss of haustra are diagnostic of ulcerative colitis.
Colonoscopic Findings
Friability and bleeding of mucosa
Continuous inflammation from rectum proximally
No skip lesions
Loss of normal vascular pattern and haustra
High-YieldNEET PG
Fecal calprotectin >250 μg/g indicates active IBD; this patient's value of 420 confirms active disease and helps exclude IBS.
Laboratory Correlation
Elevated inflammatory markers (ESR 68, CRP 12) support IBD
Microcytic anemia (Hb 9.2) from chronic blood loss
Fecal calprotectin is a neutrophil-derived protein; high levels indicate mucosal inflammation
Clinical Pearl
In ulcerative colitis, the inflammation is limited to the mucosa and submucosa, which is why extraintestinal manifestations (arthritis, uveitis, erythema nodosum) are less common than in Crohn disease.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.