A 32-year-old man with a 6-year history of ulcerative colitis (UC) presents with bloody diarrhea (8–10 stools/day), abdominal cramping, and fever (38.5°C). On examination, he is tachycardic (110/min) and has diffuse abdominal tenderness. Laboratory investigations show Hb 9.2 g/dL, WBC 14,500/μL, albumin 2.8 g/dL, and CRP 8.5 mg/dL. Sigmoidoscopy reveals continuous mucosal inflammation with ulceration and loss of haustra. What is the most appropriate immediate next step in management?
A. Start azathioprine 2 mg/kg/day as maintenance therapy
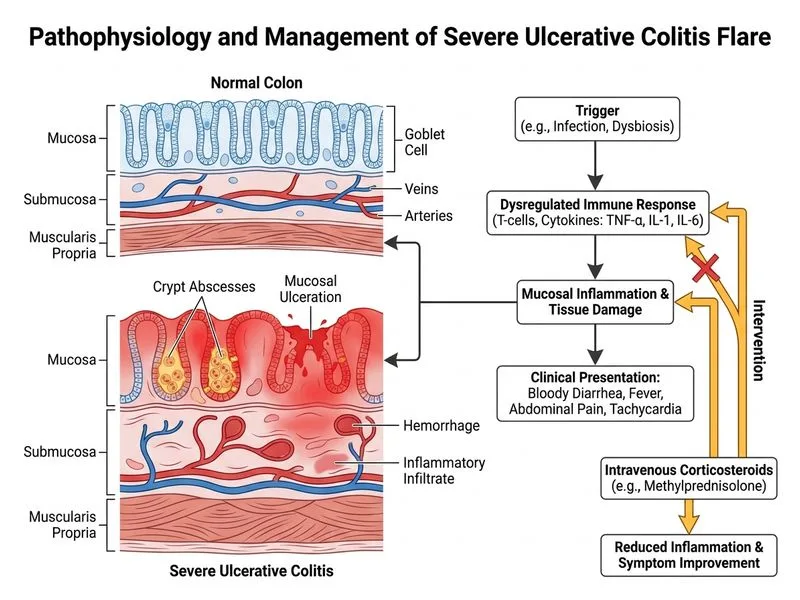
B. Initiate intravenous corticosteroids (methylprednisolone 1 g/day) and supportive care
C. Perform urgent colonoscopy with biopsy to assess disease extent and rule out malignancy
Start oral mesalamine 4.8 g/day and observe for clinical response over 1 week
D.
Explanation
Clinical Scenario Analysis
This patient presents with moderate-to-severe ulcerative colitis based on:
High stool frequency (8–10/day) with blood
Systemic signs: fever, tachycardia
Laboratory evidence of inflammation (elevated CRP, WBC) and nutritional compromise (low albumin, anemia)
Endoscopic findings: continuous inflammation with ulceration
Management Algorithm for Acute UC Exacerbation
Loading diagram...
Why Intravenous Corticosteroids?
Key Point
Moderate-to-severe UC exacerbations (≥6 stools/day + systemic toxicity) require IV corticosteroids as first-line therapy, not oral agents or biologics as monotherapy.
High-YieldNEET PG
The standard induction regimen is:
Methylprednisolone 1 g IV daily (or hydrocortisone 100 mg IV QID) for 3–5 days
Concurrent supportive measures: IV fluids, electrolyte repletion, blood transfusion for Hb <7 g/dL
Prophylactic antibiotics if signs of sepsis or toxic megacolon suspected
Clinical Pearl
Response is assessed at day 3–5:
If responding: continue IV steroids and taper over 2–3 weeks
If no response: escalate to rescue therapy (infliximab or cyclosporine)
Warning
Do NOT delay IV steroids while awaiting colonoscopy — the acute phase takes priority. Sigmoidoscopy has already confirmed the diagnosis and extent; full colonoscopy can be deferred until remission to assess for dysplasia or malignancy.