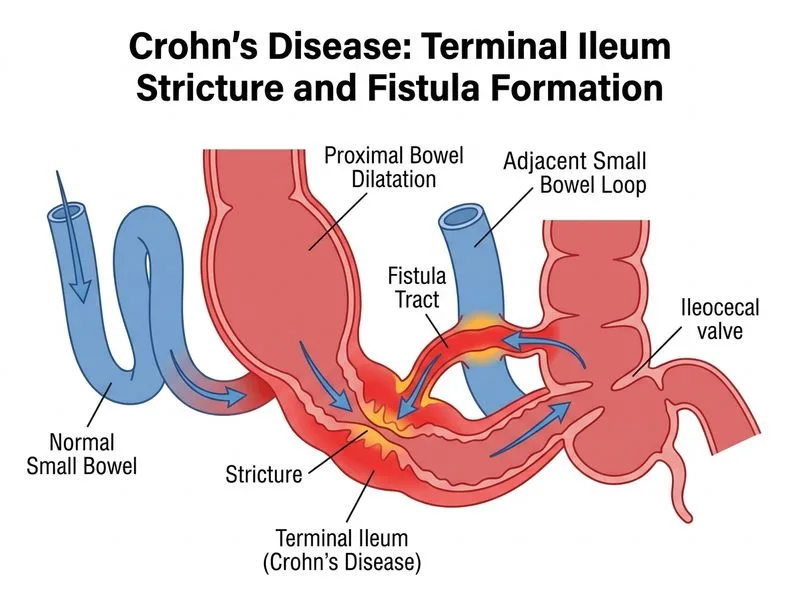
A 28-year-old woman with Crohn's disease (CD) of 8 years' duration presents with a 3-month history of progressive right lower abdominal pain, palpable mass in the right iliac fossa, and weight loss (4 kg). She is afebrile, with normal WBC and CRP. Contrast-enhanced CT abdomen shows a 6 cm stricture in the terminal ileum with proximal bowel dilatation and a small fistula to the adjacent small bowel loop. She is currently on mesalamine monotherapy. What is the most appropriate next step in management?
A. Perform double-balloon enteroscopy for stricture dilation and fistula assessment
B. Refer for surgical resection of the strictured segment with primary anastomosis
C. Increase mesalamine dose to 4.8 g/day and add oral budesonide 9 mg/day
D. Initiate infliximab induction therapy (5 mg/kg IV at weeks 0, 2, 6) and continue mesalamine
Explanation
Clinical Presentation: Structuring Crohn's Disease with Fistulization
This patient demonstrates complicated CD with:
Stricturing phenotype: 6 cm terminal ileal stricture with proximal dilatation (mechanical obstruction risk)
Fistulizing disease: small bowel-to-bowel fistula
Chronicity: 8-year disease duration with inadequate medical control on mesalamine monotherapy
Absence of active inflammation: afebrile, normal WBC, normal CRP (suggests fibrostenosing rather than inflammatory pathology)
Pathophysiology: Why Medical Therapy Fails in Stricturing Disease
Key Point
Strictures in CD are primarily fibrotic (collagen deposition and smooth muscle hypertrophy), not inflammatory. Biologics and corticosteroids target inflammation and are ineffective for established fibrotic strictures.
High-YieldNEET PG
The Montreal Classification divides CD phenotypes:
Inflammatory (B1): responsive to medical therapy
Stricturing (B2): fibrotic; medical therapy fails
Penetrating (B3): fistulizing; requires escalation or surgery
This patient has B2 + B3 (stricturing + fistulizing) disease.
Decision Algorithm: When to Operate in CD
Loading diagram...
Why Surgery Is Indicated Here
Table
Feature
Implication
6 cm stricture
Likely fibrotic; high risk of obstruction
Fistula present
Penetrating disease; medical therapy alone insufficient
Normal inflammatory markers
Suggests fibrosis, not active inflammation
Inadequate response to mesalamine
8 years on monotherapy = failed medical control
Palpable mass + symptoms
Symptomatic disease requiring intervention
Clinical Pearl
Surgery is not contraindicated in CD and is often necessary for:
Symptomatic strictures with obstruction
Fistulizing disease unresponsive to medical therapy
Perforation or abscess
Dysplasia or malignancy
Resection of the diseased terminal ileum with primary ileocolic anastomosis is the standard approach.
Why Other Options Fail
Option A (Escalate mesalamine + budesonide):
Budesonide is for inflammatory flares, not fibrotic strictures
Will not reverse established fibrosis or resolve fistula
Delays necessary surgical intervention
Option B (Infliximab induction):
Biologics are most effective for inflammatory CD
Fibrotic strictures do not respond to TNF-α inhibitors
Fistulas may respond to infliximab, but the stricture will persist
Patient already has 8 years of disease with inadequate control — escalation is unlikely to succeed
Option D (Endoscopic dilation):
Stricture is 6 cm long (too long for safe dilation)
Fistula present increases perforation risk during dilation
Temporary measure only; recurrence is high in CD
Not appropriate as primary therapy for symptomatic stricturing disease
Harrison 21e Ch 295; Robbins 10e Ch 17
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.