## Management of Difficult Cholecystectomy: Subtotal Cholecystectomy **Subtotal cholecystectomy** (leaving the gallbladder fundus in situ) is the safest approach when the CBD is densely adherent and cannot be safely dissected. ### Key Point: - **Indication**: Dense inflammation, adhesions, or fibrosis preventing safe dissection of the CBD or hepatic ducts - **Technique**: Remove the body and neck of the gallbladder; leave the fundus attached to the liver bed - **Advantage**: Avoids bile duct injury, which carries 0.3–0.7% mortality and significant morbidity - **Outcome**: Residual fundus rarely causes symptoms; recurrent stones are uncommon ### Why Intraoperative Cholangiography Doesn't Help Here: - Cholangiography identifies ductal anatomy but **does not solve the dissection problem** - The issue is **mechanical adherence**, not anatomical uncertainty - Attempting dissection after IOC increases injury risk ### Clinical Pearl: **"When in doubt, leave it out."** Subtotal cholecystectomy is preferable to a bile duct injury. Bile duct injury is a catastrophic complication requiring reoperation, ERCP, or hepaticojejunostomy. ### Comparison: | Approach | Indication | Risk | |----------|-----------|------| | **Subtotal cholecystectomy** | Dense adhesions, unclear anatomy | Minimal; residual fundus rarely symptomatic | | **CBD exploration** | Choledocholithiasis, confirmed ductal stones | Increased morbidity; not indicated here | | **Aggressive dissection** | Attempted complete removal | **High risk of bile duct injury** | 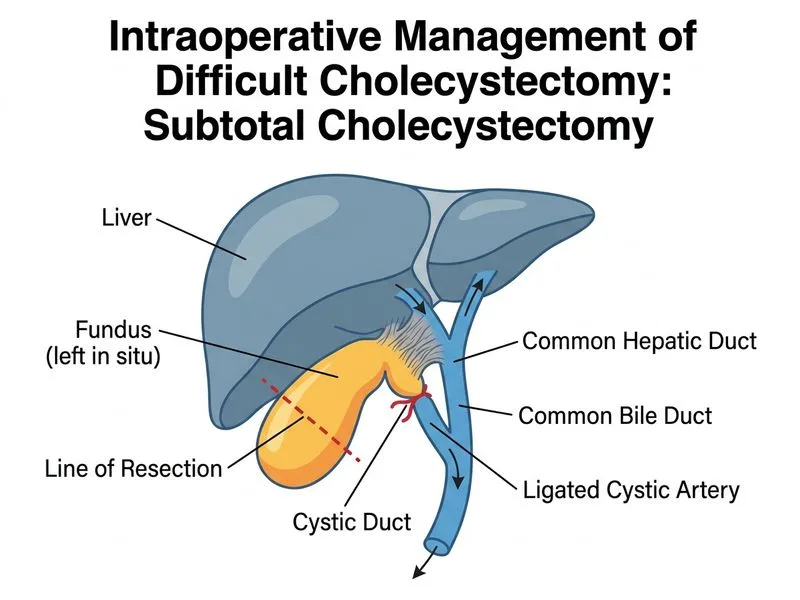
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.