Iron Deficiency Anemia MCQ — NEET PG Practice Question | NEETPGAI
Iron Deficiency Anemia
medium
microscope Pathology
A 38-year-old woman from rural Maharashtra presents with progressive fatigue, dyspnea on exertion, and palpitations for 6 months. She reports heavy menstrual bleeding for the past 2 years. On examination: pallor present, conjunctival pallor noted, no lymphadenopathy or splenomegaly. Blood investigations: Hb 7.2 g/dL, MCV 62 fL, MCH 19 pg, RBC 5.8 × 10¹²/L, serum iron 32 μg/dL (normal 60–170), TIBC 420 μg/dL (normal 250–425), ferritin 8 ng/mL (normal 12–200). Peripheral blood smear shows microcytic hypochromic RBCs with occasional target cells. What is the most likely diagnosis?
A. Iron deficiency anemia secondary to menorrhagia
B. Anemia of chronic disease
C. Sideroblastic anemia
D. Thalassemia trait
Explanation
Clinical Diagnosis: Iron Deficiency Anemia (IDA)
Key Diagnostic Features
Key Point
The combination of microcytic hypochromic anemia with low serum iron, elevated TIBC, and low ferritin in a woman with menorrhagia is pathognomonic for iron deficiency anemia.
Laboratory Interpretation
Table
Parameter
Value
Interpretation
Hb
7.2 g/dL
Moderate anemia
MCV
62 fL
Microcytic (< 80 fL)
MCH
19 pg
Hypochromic (< 27 pg)
Serum iron
32 μg/dL
Low (normal 60–170)
TIBC
420 μg/dL
Elevated (normal 250–425)
Ferritin
8 ng/mL
Diagnostic: < 12 ng/mL confirms iron deficiency
RBC count
5.8 × 10¹²/L
Elevated (paradoxically high in IDA)
High-YieldNEET PG
In iron deficiency anemia, the RBC count is often normal or elevated because the body compensates by producing more RBCs, even though each is smaller and paler. This distinguishes IDA from thalassemia, where RBC count is markedly elevated (often > 6.5 × 10¹²/L) with proportionally lower Hb.
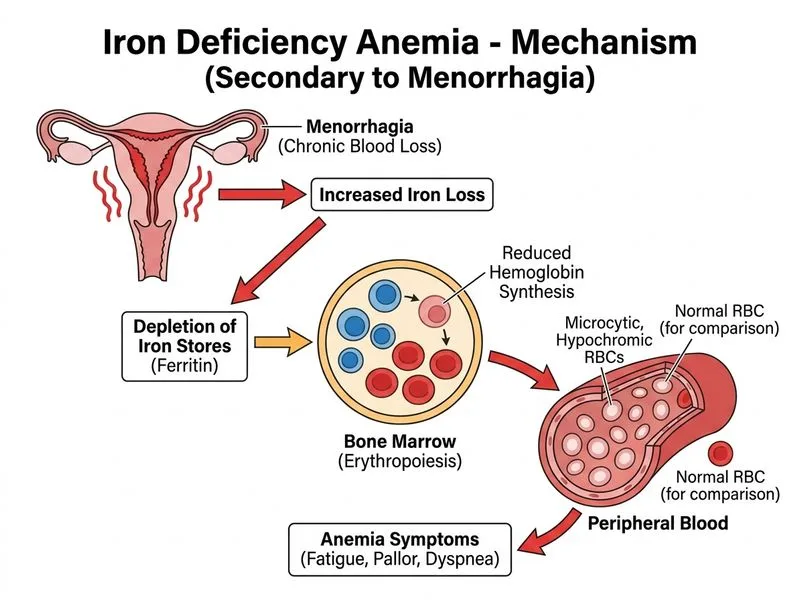
Pathophysiology of Iron Deficiency
1.
Chronic blood loss (menorrhagia) → depletion of iron stores
2.
Depleted ferritin → reduced iron availability for hemoglobin synthesis
Compensatory erythropoiesis → increased RBC production (hence RBC count may be normal or high)
5.
Peripheral smear findings:
Microcytic hypochromic RBCs (dominant)
Target cells (due to reduced hemoglobin content)
Occasional pencil cells (elliptocytes)
Anisocytosis and poikilocytosis
Iron Metabolism in IDA
Key Point
In iron deficiency, the body upregulates iron absorption and mobilization:
Serum iron ↓ (depleted body stores)
TIBC ↑ (increased transferrin synthesis to maximize iron capture)
Transferrin saturation ↓ (iron/TIBC ratio < 16%)
Ferritin ↓ (depleted iron stores; most specific marker)
Clinical Pearl
Ferritin < 12 ng/mL is diagnostic of iron deficiency in the absence of inflammation. In this patient, ferritin 8 ng/mL confirms absolute iron deficiency.
Etiology in This Patient
Menorrhagia (heavy menstrual bleeding) is the most common cause of IDA in non-pregnant women in developed countries and increasingly in India. Normal menstrual loss is 30–40 mL/cycle; menorrhagia is defined as > 80 mL/cycle. Chronic blood loss exceeds the body's ability to absorb dietary iron (~1–2 mg/day), leading to progressive depletion.
Why This Is NOT Thalassemia Trait
Warning
Thalassemia trait (β-thalassemia minor) also presents with microcytic hypochromic anemia and is common in India. However, the ferritin is normal or elevated in thalassemia (iron overload from repeated transfusions or ineffective erythropoiesis). Additionally, RBC count in thalassemia is typically > 6.5 × 10¹²/L (much higher than in IDA), and serum iron and TIBC are normal.
Mnemonic: TIBC in IDA vs. Thalassemia
IDA: Low iron, High TIBC, Low ferritin
Thalassemia: Normal iron, Normal TIBC, Normal/High ferritin
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.