| Feature | Squamous Cell Carcinoma | Adenocarcinoma |
|---|---|---|
| Location | Central (lobar/main bronchi) | Peripheral (distal airways) |
| Smoking | Strongly associated | Weakly associated |
| Metaplasia | Squamous | Mucous/glandular |
| Cavitation | Common | Rare |
| Bronchoscopy | Accessible | Often not visible |
Loading illustration…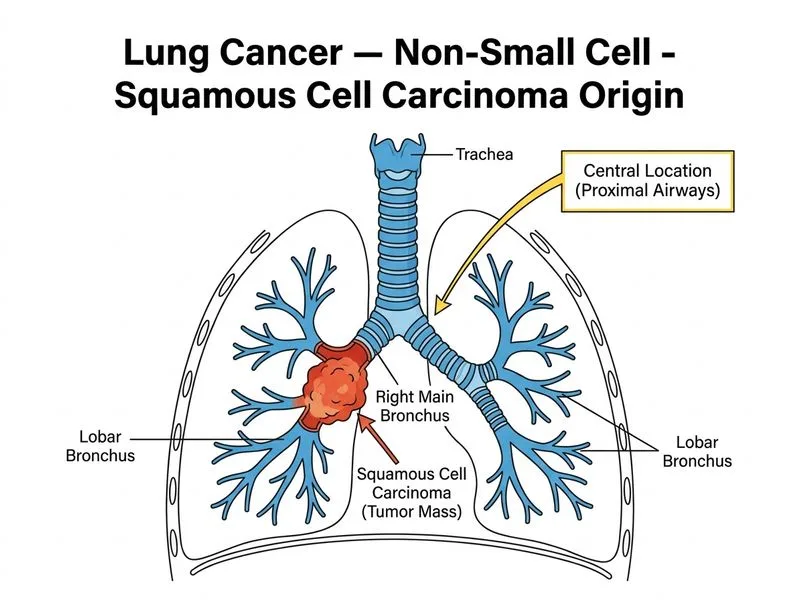
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →