A 58-year-old male smoker presents with a 3-month history of persistent cough and haemoptysis. Chest X-ray shows a 4 cm peripheral nodule in the right lower lobe with irregular margins. CT chest confirms a solitary pulmonary nodule suspicious for malignancy. What is the investigation of choice to establish histological diagnosis?
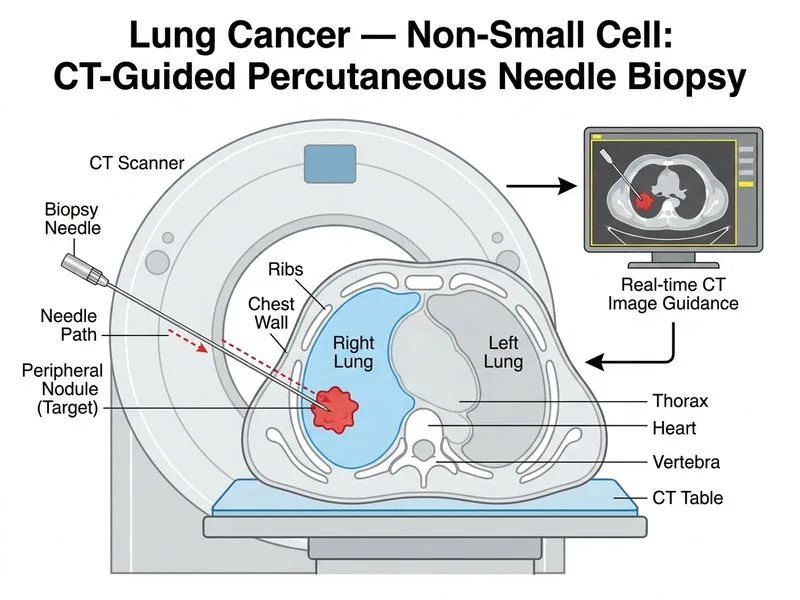
A. CT-guided percutaneous needle biopsy
B. Transthoracic needle aspiration cytology (TTNAC)
C. Bronchoscopy with brushings and washings
D. Sputum cytology
Explanation
Investigation of Choice for Peripheral Lung Nodule Diagnosis
Clinical Context
The patient has a peripheral lung nodule (4 cm, right lower lobe) suspicious for malignancy on imaging. The goal is to obtain tissue for histological diagnosis to confirm lung cancer and determine cell type (adenocarcinoma, squamous cell, etc.).
Why CT-Guided Percutaneous Needle Biopsy?
Key Point
CT-guided percutaneous needle biopsy is the gold standard for diagnosis of peripheral lung nodules >2 cm that are accessible and not in close proximity to vital structures.
High-YieldNEET PG
This technique offers:
1.
Direct visualization of the nodule under CT guidance
2.
High diagnostic yield (>90% for nodules >2 cm)
3.
Tissue procurement — allows core biopsy for histology, immunohistochemistry, and molecular testing (EGFR, ALK, PD-L1)
4.
Minimal morbidity — outpatient procedure with low complication rate
5.
Rapid diagnosis — results available within days
Comparison with Other Investigations
Table
Investigation
Indication
Yield
Limitation
CT-guided needle biopsy
Peripheral nodules >2 cm, accessible
>90%
Requires radiologist expertise
TTNAC
Peripheral nodules, high-risk patients
85–95%
Cytology only; may not subtype
Bronchoscopy
Central lesions, endobronchial disease
40–60% for peripheral
Poor yield for peripheral nodules
Sputum cytology
Screening, central airway lesions
<50%
Very low sensitivity for nodules
Clinical Pearl
TTNAC is an acceptable alternative if the nodule is >2 cm and the patient is a poor surgical candidate, but core biopsy (needle biopsy) is preferred because it provides tissue architecture and allows molecular profiling.
Molecular Testing Requirement
Key Point
In non-small cell lung cancer (NSCLC), tissue diagnosis is essential not only for histology but also for predictive molecular testing:
EGFR mutations (adenocarcinoma)
ALK rearrangements (adenocarcinoma)
PD-L1 expression (immunotherapy eligibility)
KRAS mutations (adenocarcinoma)
Cytology specimens are often insufficient for these assays; core tissue is mandatory.
Robbins 10e Ch 15
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.