Lung Cancer — Non-Small Cell MCQ — NEET PG Practice Question | NEETPGAI
Lung Cancer — Non-Small Cell
medium
microscope Pathology
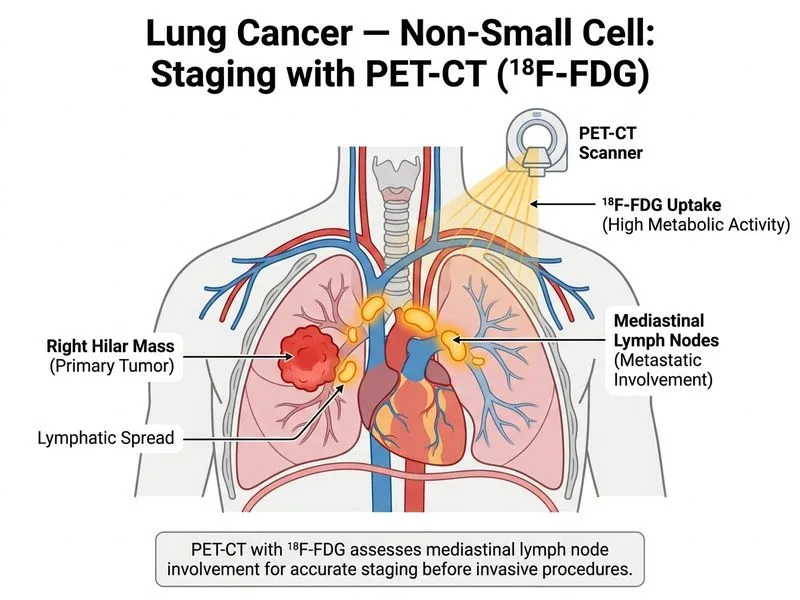
A 62-year-old woman with a history of smoking presents with chest pain and dyspnoea. Chest X-ray reveals a large right hilar mass with mediastinal widening. Bronchoscopy is planned to assess for endobronchial involvement and obtain tissue diagnosis. Which investigation should be performed BEFORE bronchoscopy to assess mediastinal lymph node involvement and guide staging?
A. Chest CT with contrast
B. Mediastinoscopy under general anaesthesia
C. Endobronchial ultrasound with transbronchial needle aspiration (EBUS-TBNA)
D. PET-CT with ¹⁸F-FDG
Explanation
Investigation for Mediastinal Assessment in NSCLC
Clinical Context
The patient has a large hilar mass with mediastinal widening, suggesting possible mediastinal lymph node involvement (N2/N3 disease). Accurate staging is critical for treatment planning (surgery vs. chemoradiation). The question asks which investigation should be performed before bronchoscopy to assess mediastinal involvement.
Why PET-CT with ¹⁸F-FDG?
Key Point
PET-CT is the single most important investigation for staging NSCLC because it provides both anatomical (CT) and functional (metabolic) information, allowing detection of mediastinal lymph node involvement and distant metastases in a single study.
High-YieldNEET PG
PET-CT advantages:
1.
Detects metabolically active lymph nodes — FDG uptake indicates malignancy (sensitivity ~85–90% for mediastinal nodes)
2.
Identifies distant metastases — bone, liver, brain, adrenal (changes staging from local to stage IV)
3.
Non-invasive — no general anaesthesia required
4.
Performed early — guides decision between surgery, chemoradiation, or palliative care
5.
Guides further invasive staging — if PET-positive mediastinal nodes, EBUS-TBNA or mediastinoscopy can be targeted