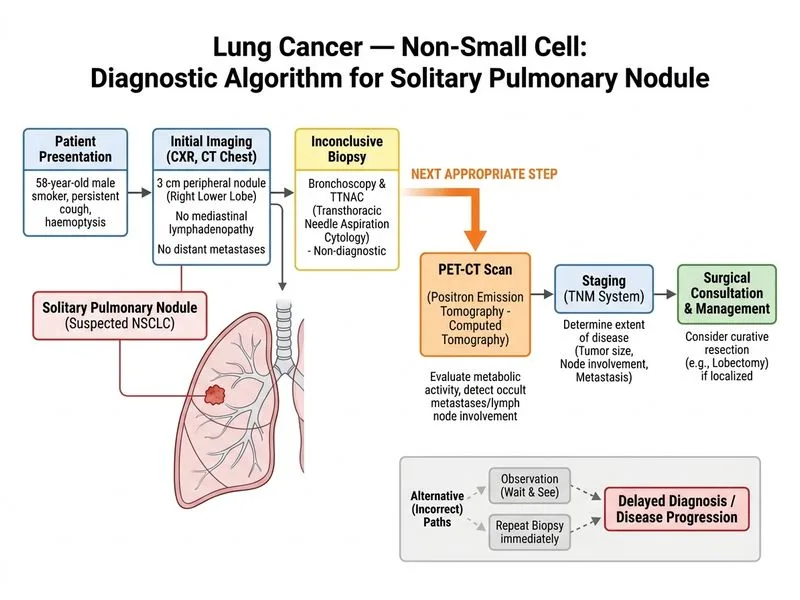
A 58-year-old male smoker presents with a 2-month history of persistent cough and haemoptysis. Chest X-ray shows a 3 cm peripheral lung nodule in the right lower lobe with no mediastinal lymphadenopathy. CT chest confirms a solitary nodule with no distant metastases. Bronchoscopy and transthoracic needle aspiration cytology (TTNAC) are inconclusive. What is the most appropriate next step in management?
A. Start empirical chemotherapy based on clinical suspicion
B. Proceed to diagnostic video-assisted thoracoscopic surgery (VATS) with wedge resection
C. Repeat TTNAC under CT guidance
D. Perform PET-CT scan followed by staging and surgical consultation
Explanation
Clinical Context
A 58-year-old male smoker with haemoptysis and a 3 cm peripheral solitary pulmonary nodule (SPN) with no mediastinal lymphadenopathy or distant metastases on CT, and inconclusive bronchoscopy + TTNAC, represents a high-probability malignancy scenario. The question asks for the best next step when non-invasive and minimally invasive sampling have both failed.
Rationale for Diagnostic VATS with Wedge Resection
Key Point
When cytological/histological sampling of a peripheral lung nodule is inconclusive after standard attempts (bronchoscopy + TTNAC), current guidelines (NCCN, BTS, ACCP) recommend surgical resection — specifically VATS wedge resection — as the next step. This approach simultaneously achieves:
Curative resection if malignancy is confirmed (converted to lobectomy if needed)
3.
Avoidance of further diagnostic delay in a high-risk patient
High-YieldNEET PG
For a peripheral nodule ≥2 cm in a high-risk smoker with inconclusive prior sampling, VATS wedge resection is both diagnostic AND potentially therapeutic in a single procedure. This is the standard of care per ACCP Evidence-Based Clinical Practice Guidelines (Chest 2013) and NCCN NSCLC guidelines.
Why Not the Other Options?
Option A (Repeat CT-guided TTNAC): TTNAC has already been performed and was inconclusive. Repeating it carries additional risk (pneumothorax ~15–25%) with a significant chance of another non-diagnostic result, especially for peripheral nodules with necrotic or heterogeneous tissue. Guidelines do not recommend routine repeat sampling when surgical resection is feasible.
Option C (Empirical chemotherapy): Absolutely contraindicated without tissue diagnosis. "Tissue before treatment" is a cardinal oncology principle. Starting chemotherapy without histological confirmation violates standard of care.
Option D (PET-CT followed by staging): PET-CT is valuable for staging after a tissue diagnosis is established, or when the pre-test probability of malignancy is intermediate and non-invasive characterisation may change management. In this case, the patient already has a high-probability malignant nodule with no CT evidence of metastases, and two sampling attempts have failed. PET-CT would add delay without providing the tissue diagnosis needed to guide treatment. Moreover, if PET-CT shows no metastases, VATS would still be required — making it an unnecessary intermediate step.
Management Algorithm for Inconclusive Sampling of High-Risk SPN
The principle of "one-stop diagnosis and treatment" via VATS is preferred over repeated failed sampling or staging investigations that delay definitive management in a surgically fit patient with a resectable lesion.
ACCP Evidence-Based Clinical Practice Guidelines, Chest 2013; NCCN NSCLC Guidelines v2024; Harrison's Principles of Internal Medicine 21e, Ch 89
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.