A 62-year-old woman with limited-stage small cell lung cancer (LD-SCLC) has completed 4 cycles of concurrent cisplatin–etoposide chemotherapy and thoracic radiotherapy (45 Gy in 30 fractions). Restaging CT chest shows complete response of the primary tumor and mediastinal nodes. Brain MRI is normal. She is asymptomatic. What is the most appropriate next step in management?
A. Observation with 3-monthly clinical follow-up and imaging
B. Palliative whole-brain radiotherapy
C. Adjuvant topotecan chemotherapy
D. Prophylactic cranial irradiation (PCI)
Explanation
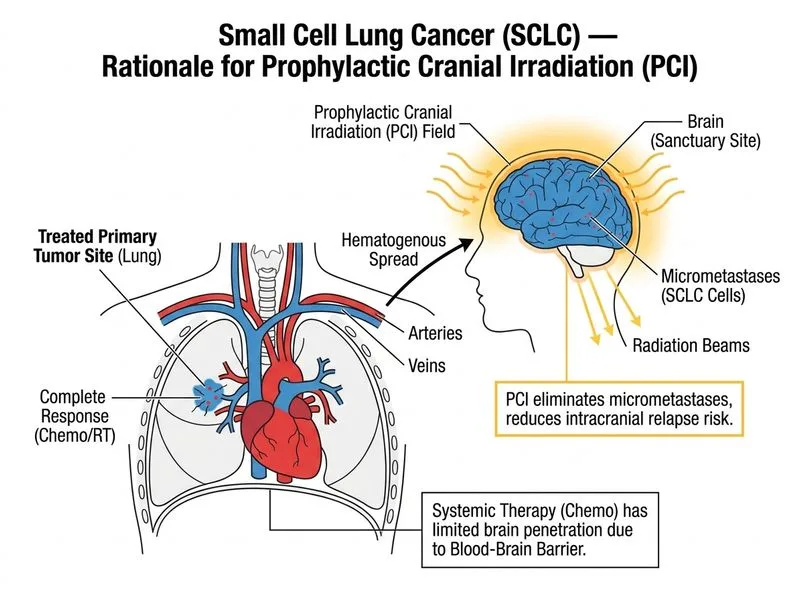
Prophylactic Cranial Irradiation (PCI) in Limited-Stage SCLC
Key Point
Prophylactic cranial irradiation (PCI) is the standard of care for patients with limited-stage SCLC who achieve a complete or good partial response to initial chemoradiotherapy. It reduces the cumulative incidence of brain metastases from 40% to 15% and improves overall survival by ~5%.
Evidence and Rationale
High-YieldNEET PG
The landmark trial (Aupérin et al., 1999) demonstrated that PCI in SCLC patients with complete response reduces brain relapse risk and improves 3-year overall survival (15% → 20.7%). This benefit is seen across both limited-stage and extensive-stage disease.
Clinical Pearl
SCLC has a natural propensity for CNS sanctuary disease due to:
High growth fraction and early hematogenous dissemination
Chemotherapy and radiotherapy penetration into the brain is limited
Microscopic disease in the brain is present in ~25% of patients at diagnosis despite negative MRI
Timing and Technique
Mnemonic
PCI = Post-Chemoradio Intervention — delivered after completion of chemotherapy and thoracic radiotherapy, typically within 4–6 weeks of completing systemic treatment.
Dose: 25 Gy in 10 fractions (standard) or 30 Gy in 12 fractions
Timing: Within 4–6 weeks of completing chemotherapy (while disease control is optimal)
Indication: Complete or near-complete response to induction therapy
Confusing PCI (prophylactic, in responders) with therapeutic WBRT (in patients with brain metastases)
Omitting PCI in LD-SCLC responders—this significantly worsens prognosis
Why Other Options Are Incorrect
Observation alone: Without PCI, ~40% of LD-SCLC patients will develop brain metastases within 2 years, leading to poor quality of life and shortened survival. Observation is not standard of care after complete response.
Adjuvant topotecan: There is no evidence for maintenance or adjuvant chemotherapy in SCLC after complete response to induction therapy. Topotecan is used for relapsed disease, not consolidation.
Therapeutic WBRT: Reserved for patients with symptomatic or imaging-detected brain metastases, not for prophylaxis in asymptomatic patients.
Harrison 21e Ch 111; NCCN Guidelines on Small Cell Lung Cancer
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.