A 28-year-old man presents with a 3-week history of painless lymphadenopathy in the neck and mediastinal fullness on chest X-ray. Excisional lymph node biopsy is planned. Which investigation is most appropriate to confirm the diagnosis of Hodgkin lymphoma and determine histological subtype?
A. Serum LDH and ESR measurement
B. PET-CT scan of the chest and abdomen
C. Flow cytometry of lymph node aspirate
D. Histopathology with immunohistochemistry of excised lymph node
Explanation
Diagnostic Confirmation in Hodgkin Lymphoma
Key Point
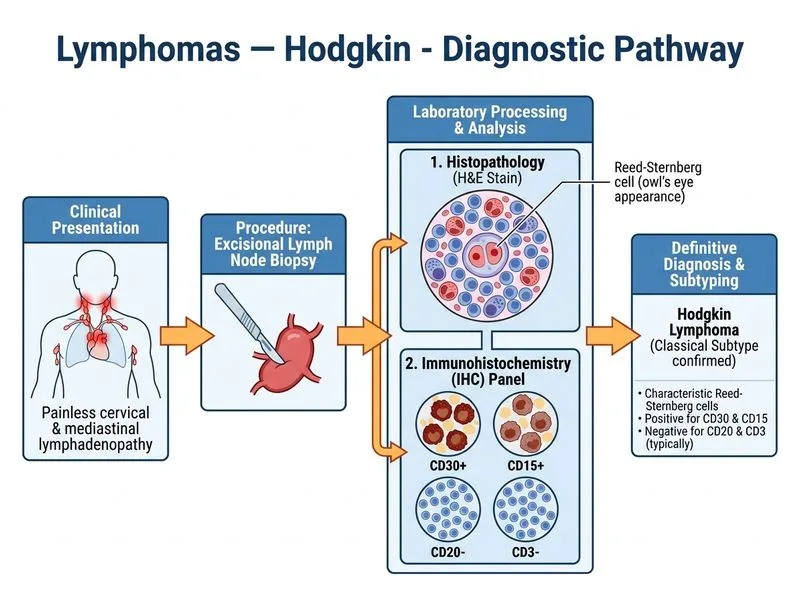
Histopathology with immunohistochemistry (IHC) of excised lymph node tissue is the gold standard for diagnosis and subtype classification of Hodgkin lymphoma.
Why Histopathology + IHC is Definitive
1.
Morphological identification of diagnostic cells:
Reed-Sternberg (RS) cells — large multinucleated cells with "owl's eye" nuclei
Hodgkin cells — mononuclear variants
Background of small lymphocytes, eosinophils, and plasma cells
2.
Immunophenotype confirmation:
CD30+, CD15+ (RS/Hodgkin cells)
CD45−, CD20− (typically B-cell marker negative)
CD3− (T-cell marker negative)
3.
Histological subtype classification (essential for prognosis and treatment):
Nodular sclerosis (most common, ~70%)
Mixed cellularity (~15%)
Lymphocyte-rich (~5%)
Lymphocyte-depleted (rare, ~1%)
High-YieldNEET PG
The combination of morphology + IHC phenotype is diagnostic; neither alone is sufficient. Excisional biopsy (not needle core) is preferred because it preserves tissue architecture needed to assess background cellularity and fibrosis.
Investigation Hierarchy
Table
Investigation
Role
Diagnostic?
Histopathology + IHC
Definitive diagnosis + subtype
YES
Flow cytometry
Useful in lymphoid neoplasms; poor for HL (sparse RS cells)
No
Serum LDH, ESR
Prognostic markers, not diagnostic
No
PET-CT
Staging and treatment response; not diagnostic
No
Clinical Pearl
Flow cytometry is often unhelpful in Hodgkin lymphoma because RS cells are sparse in the background of reactive cells, making them difficult to gate and identify by flow alone. Tissue architecture is critical.