A 38-year-old Indian woman presents with a 2-month history of painless left inguinal lymphadenopathy and intermittent fever. Physical examination reveals a 4 cm firm, matted lymph node in the left groin and no hepatosplenomegaly. Laboratory investigations show hemoglobin 11.5 g/dL, WBC 7,200/μL, and platelets 180,000/μL. Excisional lymph node biopsy shows effacement of normal architecture with a nodular growth pattern. Histology reveals small lymphocytes and scattered large cells with clear cytoplasm and prominent nucleoli. Immunohistochemistry shows CD20+, CD10+, BCL2+, and BCL6+ large cells. What is the most likely diagnosis?
A. Diffuse large B-cell lymphoma
B. Primary mediastinal B-cell lymphoma
C. Burkitt lymphoma
Follicular lymphoma
D.
Explanation
Diagnosis: Follicular Lymphoma (Grade I–II)
Clinical Presentation
The patient presents with:
Painless lymphadenopathy (inguinal node)
Systemic symptoms (fever)
No hepatosplenomegaly
Normal blood counts
Young to middle-aged woman
Key Point
Follicular lymphoma is the second most common B-cell lymphoma worldwide. It typically presents with nodal disease, often in advanced stage (stage III–IV), but with preserved performance status and normal cytopenias.
Histopathology — The Diagnostic Hallmark
Nodular growth pattern with:
Neoplastic germinal centers composed of:
Centrocytes (small cleaved cells with irregular nuclei)
Centroblasts (large cells with vesicular nuclei and prominent nucleoli)
Preserved mantle zone at periphery
Small lymphocytes in interfollicular areas
High-YieldNEET PG
The nodular pattern of follicular lymphoma is distinct from the diffuse infiltration seen in other lymphomas. The presence of both small centrocytes and larger centroblasts within germinal center-like structures is pathognomonic.
Immunophenotype — B-Cell Germinal Center Signature
Table
Feature
Follicular
DLBCL
Burkitt
Primary Mediastinal
CD20
Positive
Positive
Positive
Positive
CD10
Positive
Negative (except GCB type)
Negative
Negative
BCL2
Positive
Negative (usually)
Negative
Negative
BCL6
Positive
Positive (GCB type)
Negative
Negative
CD5
Negative
Negative
Negative
Negative
MYC translocation
Negative
Negative (usually)
t(8;14)
Negative
t(14;18)
Present (85%)
Absent
Absent
Absent
Mnemonic
Follicular = CD10 + BCL2 + t(14;18) — "Follicular has Four features: germinal center origin (CD10+), anti-apoptosis (BCL2+), and the t(14;18) translocation."
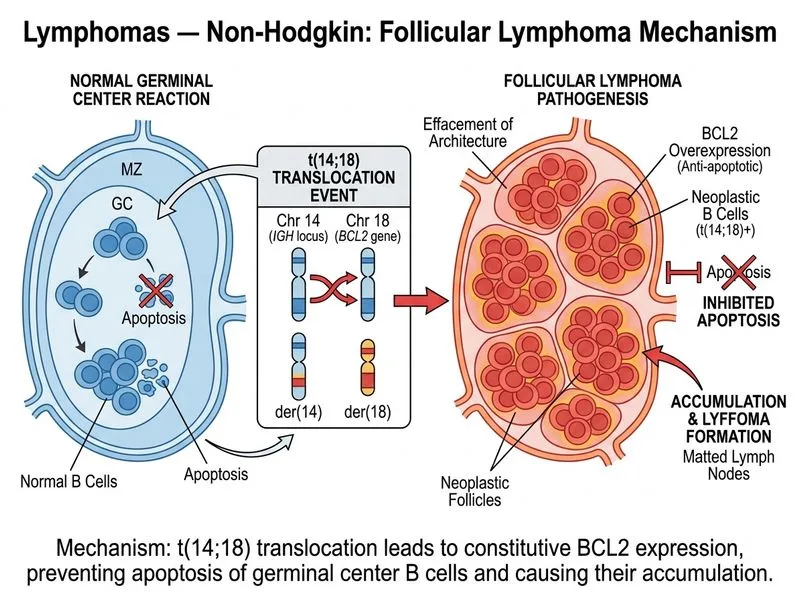
Molecular Hallmark
t(14;18)(q32;q21) juxtaposes BCL2 (chromosome 18) to the immunoglobulin heavy chain (IGH) locus (chromosome 14), resulting in constitutive BCL2 expression and resistance to apoptosis. This translocation is present in ~85% of follicular lymphomas and is virtually absent in other lymphomas.
Clinical Pearl
The presence of BCL2+ large cells (centroblasts) in a nodular pattern with CD10+ and BCL6+ phenotype is virtually diagnostic of follicular lymphoma. The t(14;18) translocation can be detected by fluorescence in situ hybridization (FISH) or PCR.
Grading
Follicular lymphomas are graded by the number of centroblasts per high-power field (hpf):
Grade I: 0–5 centroblasts/hpf
Grade II: 6–15 centroblasts/hpf
Grade III: >15 centroblasts/hpf (subdivided into IIIA and IIIB)
This case, with scattered large cells and preserved nodular architecture, suggests Grade I–II follicular lymphoma.
Why This Is Follicular Lymphoma and Not Other Lymphomas
Diffuse large B-cell lymphoma (DLBCL) would show:
Diffuse infiltration (not nodular)
Predominantly large cells (>50% of cellularity)
CD10+ only in germinal center B-cell (GCB) subtype; BCL2 usually negative
Often presents with B symptoms and rapid progression
Higher grade, more aggressive course
Burkitt lymphoma would show:
Diffuse infiltration with monomorphous medium-sized blasts
Starry-sky pattern (macrophages with tingible bodies)
CD10+, but BCL2− (no t(14;18))
t(8;14) translocation (MYC rearrangement)
Extremely aggressive, presents with high tumor burden
Young patients, often with extranodal disease
Primary mediastinal B-cell lymphoma would show:
Mediastinal mass (not peripheral lymph node)
Sclerotic fibrosis and compartmentalization
CD20+, but CD10−, BCL2−
Often presents with chest symptoms or superior vena cava syndrome
Young women typically affected
High-YieldNEET PG
The nodular pattern + CD10+ + BCL2+ + t(14;18) triad is diagnostic of follicular lymphoma and excludes all other options.
Clinical Course & Prognosis
Indolent course with median overall survival of 8–10 years (without treatment)
Often presents in advanced stage (III–IV) but with good performance status
Risk of Richter transformation to DLBCL (~3–5% per year)
Incurable with conventional chemotherapy; watch-and-wait is often appropriate for asymptomatic patients
Follicular lymphoma is a "watch-and-wait" disease in asymptomatic patients. Treatment is indicated for symptomatic disease, cytopenias, or rapid progression.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.