This patient presents with B symptoms (fever, night sweats), lymphadenopathy, hepatosplenomegaly, elevated LDH, and mediastinal involvement — a classic presentation suggestive of non-Hodgkin lymphoma (NHL), likely a high-grade subtype given the constitutional symptoms.
Fine-needle aspiration (FNA) is inadequate for lymphoma diagnosis because it cannot assess tissue architecture, which is essential for subtype classification. Excisional biopsy of the most accessible lymph node (avoiding small nodes <1 cm) is preferred.
Once histology confirms NHL, staging investigations (CT, PET-CT, bone marrow biopsy if indicated) follow to determine extent of disease and prognosis — but only after tissue diagnosis is secured.
Loading illustration…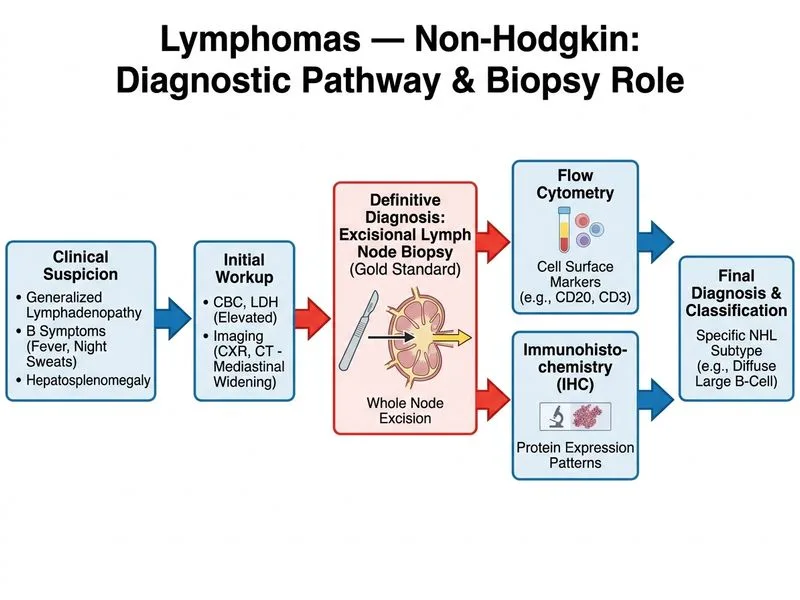
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →