A 42-year-old woman from Mumbai is found to have a solitary 2 cm right axillary lymph node on routine examination. She is asymptomatic with normal hemoglobin, WBC, and platelets. LDH is normal. Excisional biopsy confirms follicular lymphoma, grade 1–2. CT chest, abdomen, and pelvis shows no other lymphadenopathy or organ involvement. Bone marrow biopsy is negative. What is the most appropriate next step in management?
A. Immediate rituximab monotherapy
B. Rituximab-cyclophosphamide-doxorubicin-vincristine-prednisolone (R-CHOP) chemotherapy
C. Radiation therapy to the axilla followed by systemic chemotherapy
D. Observation with clinical and radiologic surveillance every 3 months
Explanation
Clinical Staging and Risk Stratification
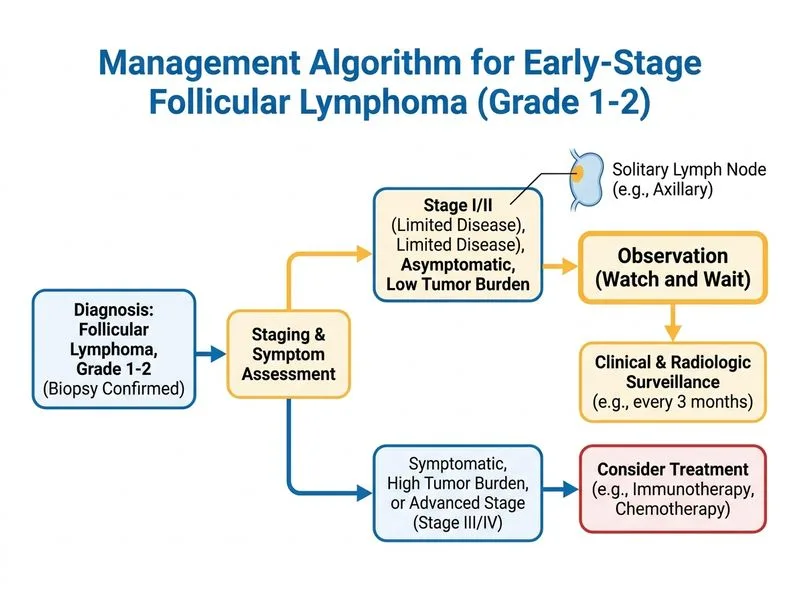
This patient has stage IA follicular lymphoma (single lymph node, no systemic involvement, normal LDH, no B symptoms). This is a low-grade, indolent NHL with an excellent prognosis.
The "Watch and Wait" Paradigm
Key Point
Early-stage, asymptomatic, low-grade NHL (especially follicular lymphoma) does NOT require immediate treatment. Observation with surveillance is the standard of care and does not compromise long-term outcomes.
High-YieldNEET PG
The "watch and wait" or "observation" strategy is supported by multiple randomized trials (e.g., GELA, PRIMA-HL) showing that:
Delaying treatment in asymptomatic patients does not worsen overall survival
Treatment can be deferred until disease progression (new lymphadenopathy, B symptoms, cytopenias, rising LDH)
Patients benefit from a treatment-free interval and avoid early chemotoxicity
Surveillance Protocol
Table
Interval
Assessment
Every 3 months (first 2 years)
Clinical exam, CBC, LDH
Every 6 months (years 2–5)
Clinical exam, CBC, LDH
Annually (after year 5)
Clinical exam, CBC, LDH
As needed
Imaging (CT/PET) if symptoms or lab abnormalities develop
Clinical Pearl
Follicular lymphoma is incurable with current standard therapy, but median overall survival exceeds 15–20 years. Early treatment does not prolong survival and exposes patients to unnecessary toxicity.
Why Not Treat Now?
Rituximab monotherapy (option 1) may be considered for symptomatic or progressive disease, not asymptomatic stage I disease.
R-CHOP (option 2) is reserved for symptomatic, progressive, or high-grade disease; it is overtreatment for asymptomatic stage IA follicular lymphoma.
Radiation therapy (option 3) is rarely used in modern NHL management and is not indicated for asymptomatic stage I disease.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.