Which of the following is the PRIMARY mechanism of airway obstruction in meconium aspiration syndrome?
A. Surfactant inactivation leading to atelectasis
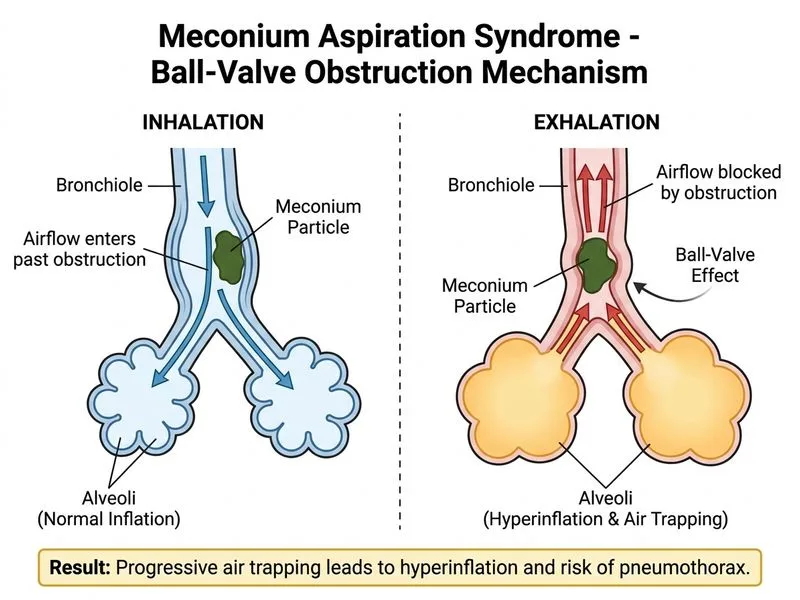
B. Ball-valve obstruction causing air trapping and hyperinflation
C. Pulmonary edema secondary to aspiration
D. Direct chemical pneumonitis from meconium constituents
Explanation
Pathophysiology of Meconium Aspiration Syndrome
Primary Mechanism
Key Point
Ball-valve obstruction is the PRIMARY and most characteristic mechanism in MAS. Meconium particles lodge at the level of terminal and respiratory bronchioles, acting as one-way valves — air enters during inspiration but cannot exit during expiration, leading to air trapping, hyperinflation, and subsequent barotrauma.
Secondary Mechanisms
While surfactant inactivation and chemical pneumonitis DO occur in MAS, they are secondary phenomena:
Table
Mechanism
Timing
Clinical Significance
Ball-valve obstruction
Immediate (first hours)
Hyperinflation, air leaks, barotrauma
Surfactant inactivation
Hours to days
Persistent atelectasis, increased work of breathing
Chemical pneumonitis
24–72 hours
Inflammation, increased airway reactivity
Pulmonary edema
Variable
Contributes to oxygenation failure
Clinical Correlates
High-YieldNEET PG
The ball-valve mechanism explains why MAS infants present with:
Barrel-shaped chest (hyperinflation)
Flattened diaphragm on CXR
Air leak syndromes (pneumothorax, pneumomediastinum) — seen in 20–40% of severe MAS
Patchy atelectasis alternating with hyperinflated zones ("classic" appearance)
Clinical Pearl
Ventilation strategies in MAS must account for air trapping — permissive hypercapnia and gentle ventilation are preferred over aggressive hyperventilation, which worsens air leaks.
Nelson Textbook of Pediatrics 21e Ch 102
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.