A 2-hour-old male neonate born to a 28-year-old primigravida at 38 weeks gestation presents with respiratory distress. The delivery was complicated by thick meconium-stained amniotic fluid (MSAF). The infant required vigorous suctioning of the oropharynx and nasopharynx at delivery. Apgar scores were 7 at 1 minute and 9 at 5 minutes. Currently, the baby has a respiratory rate of 68/min, mild intercostal retractions, and oxygen saturation of 88% on room air. Chest X-ray shows hyperinflation with patchy infiltrates and areas of atelectasis. Blood gas analysis reveals pH 7.28, PaCO₂ 52 mmHg, PaO₂ 65 mmHg on room air. Which of the following is the most appropriate initial management?
A. Immediate intubation and mechanical ventilation with high peak inspiratory pressures
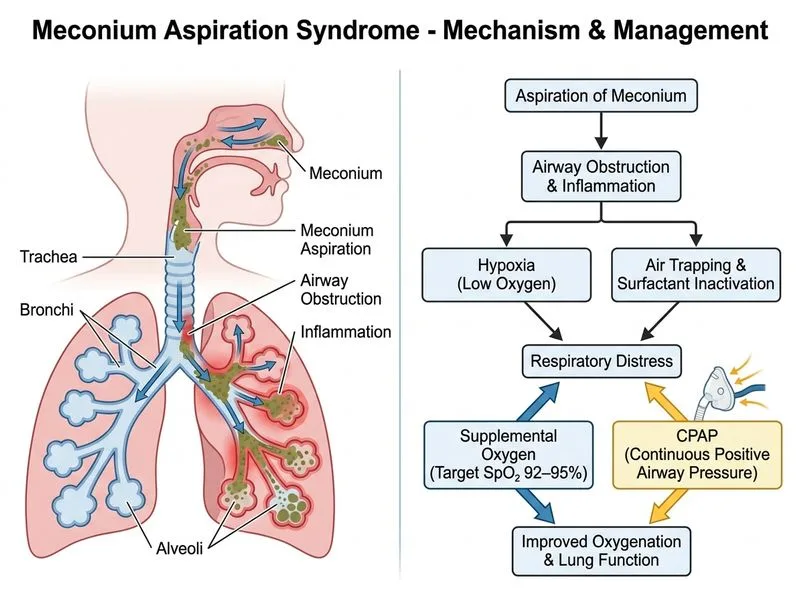
B. Supplemental oxygen to target SpO₂ 92–95% and continuous positive airway pressure (CPAP)
Surfactant replacement therapy followed by observation
C.
D. Antibiotics and supportive care without respiratory support
Explanation
Clinical Context
This is a classic presentation of Meconium Aspiration Syndrome (MAS) — a neonatal respiratory disorder caused by inhalation of meconium-stained amniotic fluid in utero or at delivery, leading to airway obstruction, inflammation, and surfactant inactivation.
Pathophysiology of MAS
Key Point
MAS results from three main mechanisms:
1.
Mechanical obstruction — meconium plugs distal airways → air trapping and hyperinflation
2.
Chemical pneumonitis — meconium components (bile acids, enzymes) damage epithelium
3.
Surfactant inactivation — meconium impairs surfactant function → atelectasis
Intact Apgar scores (9 at 5 min) — not severely depressed
CPAP provides:
Positive end-expiratory pressure (PEEP) to recruit collapsed alveoli and prevent atelectasis
Reduced work of breathing
Avoidance of intubation and ventilator-associated complications
Supplemental oxygen targets SpO₂ 92–95% (not >95%, to avoid oxygen toxicity and retinopathy of prematurity risk).
When to Escalate to Mechanical Ventilation
Key Point
Indications for intubation in MAS:
SpO₂ <85% despite CPAP + FiO₂ >0.6
PaCO₂ >55 mmHg with worsening acidosis
Severe respiratory distress with intercostal/subcostal retractions
Apnea or gasping
Pneumothorax
Clinical Pearl
Exogenous surfactant (e.g., poractant alfa) may be considered in intubated infants with MAS, as meconium inactivates endogenous surfactant. However, this patient is not yet intubated.
Role of Suctioning
Warning
Routine endotracheal intubation and suctioning of vigorous meconium-stained infants is no longer recommended (per 2015 ILCOR/AHA guidelines). This patient had appropriate oropharyngeal/nasopharyngeal suctioning at delivery. Further aggressive suctioning is not indicated unless the airway is obstructed.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.