A 6-hour-old female neonate born at 39 weeks gestation to a 32-year-old mother presents with progressive respiratory distress. Delivery was vaginal with thick meconium-stained amniotic fluid. The infant required bag-and-mask ventilation at birth (Apgar 5 at 1 min, 8 at 5 min). She was started on CPAP with FiO₂ 0.4 but has worsened over the past 2 hours. Current vital signs: RR 82/min, severe intercostal and subcostal retractions, SpO₂ 82% on CPAP with FiO₂ 0.6, HR 165/min. Chest X-ray shows hyperinflation, patchy consolidation, and a **right-sided pneumothorax**. Arterial blood gas: pH 7.18, PaCO₂ 68 mmHg, PaO₂ 58 mmHg. What is the most appropriate next step in management?
A. Immediate chest tube placement without intubation
B. Intubation and mechanical ventilation with high peak inspiratory pressures to re-expand the lung
C. Continue CPAP with increase in FiO₂ to 1.0 and observe for spontaneous reabsorption
D. Needle aspiration of pneumothorax followed by intubation, mechanical ventilation, and chest tube placement
Explanation
Clinical Context
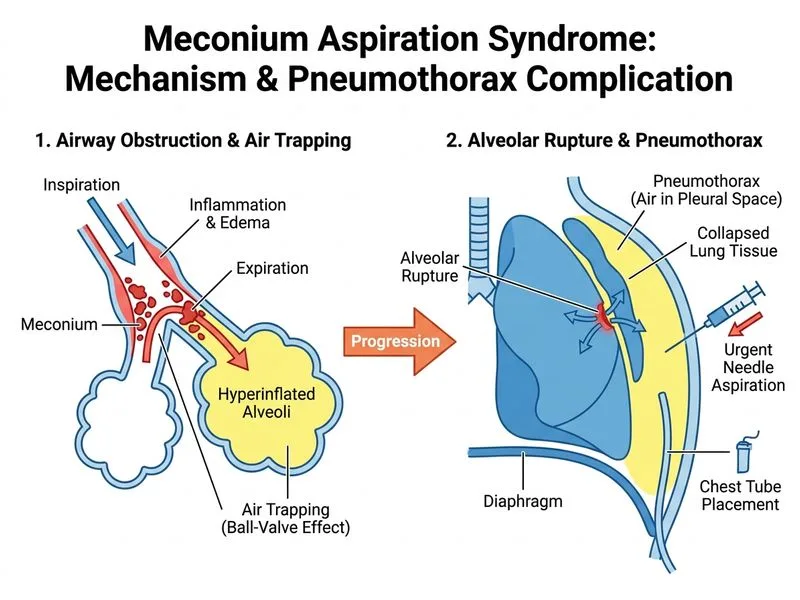
This is a complicated presentation of Meconium Aspiration Syndrome (MAS) with secondary pneumothorax — a life-threatening complication requiring urgent intervention. The infant has failed CPAP therapy and developed a tension physiology.
Why This Infant Has Worsened
Table
Finding
Mechanism
Progressive RR (82/min), severe retractions
Increased work of breathing; CPAP inadequate
SpO₂ 82% on CPAP + FiO₂ 0.6
Refractory hypoxemia
PaCO₂ 68, pH 7.18
Severe respiratory acidosis
Pneumothorax on CXR
Air leak from over-distended alveoli (barotrauma from MAS + CPAP)
HR 165/min
Compensatory tachycardia; possible tension physiology
Key Point
Pneumothorax in MAS occurs due to ball-valve obstruction by meconium → air trapping → alveolar rupture → pneumothorax. This is a known complication in ~5–10% of MAS cases.
Management of Pneumothorax in MAS
Loading diagram...
Why Needle Aspiration First?
High-YieldNEET PG
In a symptomatic, deteriorating infant with pneumothorax:
1.
Needle aspiration (22–24 G needle into 2nd intercostal space, midclavicular line) provides immediate relief of tension physiology
2.
Allows time for intubation preparation without further deterioration