A term newborn born to a mother with thick meconium-stained amniotic fluid is noted to have tachypnea (RR 68/min), grunting, and intercostal retractions within 2 hours of birth. Oxygen saturation is 88% on room air. Which investigation is most appropriate to confirm the diagnosis of meconium aspiration syndrome and assess severity?
A. Blood gas analysis
B. Chest X-ray
C. Tracheal aspirate culture
D. Meconium staining index
Explanation
Role of Chest X-ray in Meconium Aspiration Syndrome
Key Point
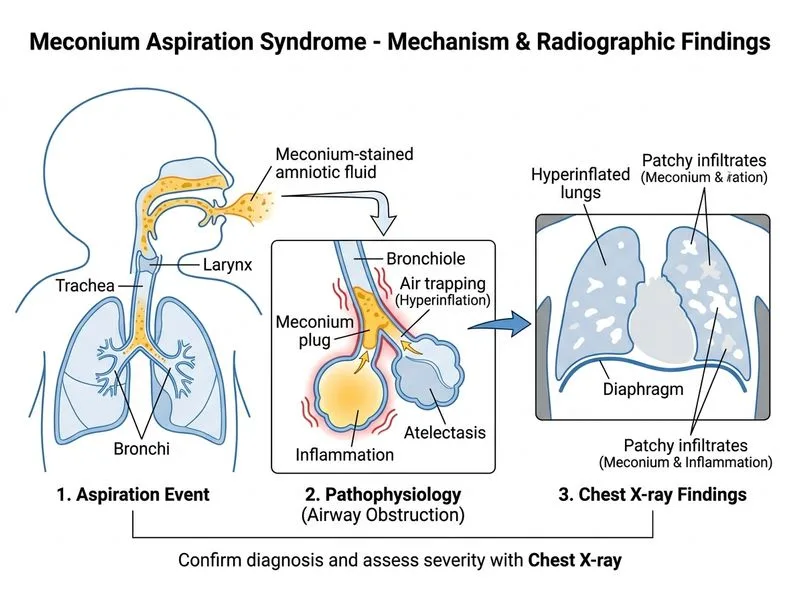
Chest X-ray is the investigation of choice for confirming meconium aspiration syndrome (MAS) and assessing the severity of pulmonary involvement.
Radiological Features of MAS
The classic findings on chest X-ray include:
1.
Patchy infiltrates — irregular, non-segmental opacities distributed throughout both lungs
2.
Hyperinflation — flattened diaphragm, increased anteroposterior diameter, and hyperlucency
3.
Air trapping — areas of atelectasis alternating with emphysema ("ball-valve" obstruction)
4.
Pneumothorax or pneumomediastinum — barotrauma from air trapping (present in ~10–15% of cases)
5.
Meconium plugging — linear or nodular opacities representing aspirated meconium
Why CXR Is Diagnostic
Confirms aspiration: The combination of clinical presentation (respiratory distress in a meconium-stained infant) + characteristic CXR findings is diagnostic of MAS
Assesses severity: Extent of infiltrates and hyperinflation correlates with disease severity and need for escalation of respiratory support
Detects complications: Identifies barotrauma (pneumothorax, pneumomediastinum) that may require urgent intervention
Guides management: Helps differentiate MAS from other causes of neonatal respiratory distress (RDS, TTN, pneumonia)
Severity Grading on CXR
Table
Grade
Features
Clinical Correlation
Mild
Patchy infiltrates, minimal hyperinflation
Mild respiratory distress, responds to supplemental O₂
Moderate
Diffuse infiltrates, moderate hyperinflation
Moderate distress, may need CPAP/mechanical ventilation
Severe
Extensive infiltrates, severe hyperinflation, barotrauma
Severe distress, high risk of air leak, requires aggressive support
High-YieldNEET PG
CXR is performed within the first 2–4 hours of life in any term or post-term infant with meconium staining and respiratory distress. It is the single best investigation to confirm diagnosis and guide therapy escalation.
Clinical Pearl
A normal CXR does NOT exclude MAS if clinical suspicion is high; mild disease may have subtle findings. Repeat imaging may be needed if clinical deterioration occurs.
Why Other Options Are Incorrect
Blood gas analysis: Useful for assessing severity (hypoxemia, hypercarbia, acidosis) and monitoring response to therapy, but does NOT confirm the diagnosis of MAS. It is a supportive investigation, not diagnostic.
Meconium staining index: This is an antenatal assessment tool (not a postnatal investigation) used to quantify meconium in amniotic fluid; it does not diagnose neonatal MAS.
Tracheal aspirate culture: Used to identify secondary bacterial infection, not to diagnose MAS. Culture results take 48–72 hours and are not useful for acute diagnosis.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.