A 6-hour-old post-term newborn with meconium aspiration syndrome on supplemental oxygen shows persistent hypoxemia (SpO₂ 85% on 60% FiO₂) and hypercarbia (PaCO₂ 58 mmHg). The neonatologist suspects pulmonary hypertension secondary to MAS. Which investigation is most appropriate to assess right ventricular function and estimate pulmonary artery pressure?
A. Echocardiography
B. Cardiac catheterization
C. Computed tomography of the chest
D. Pulmonary function testing
Explanation
Echocardiography in MAS-Associated Pulmonary Hypertension
Key Point
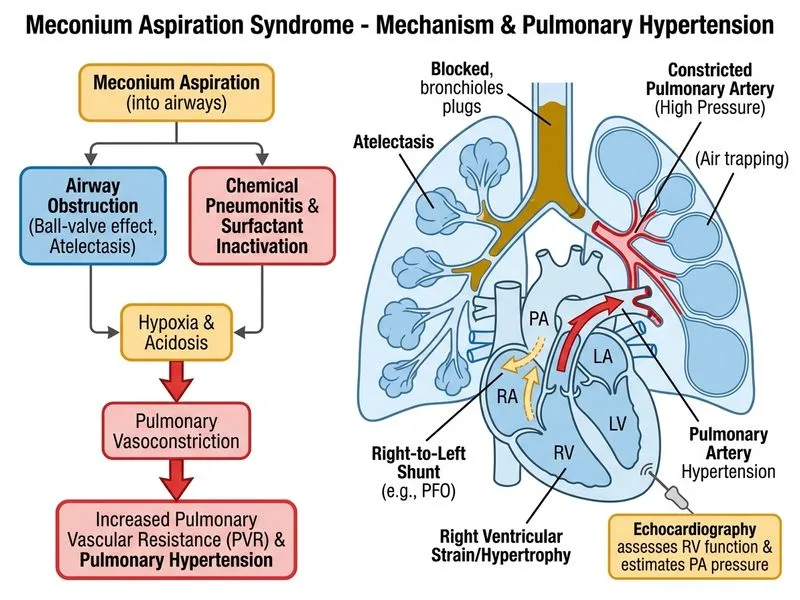
Echocardiography is the investigation of choice for assessing right ventricular function, estimating pulmonary artery pressure, and detecting pulmonary hypertension in neonates with severe meconium aspiration syndrome.
Pathophysiology of Pulmonary Hypertension in MAS
Meconium aspiration causes:
1.
Airway obstruction → air trapping → increased intrathoracic pressure
2.
Hypoxemia and hypercarbia → pulmonary vasoconstriction
3.
Inflammation → release of vasoactive mediators (endothelin, leukotrienes)
4.
Increased pulmonary vascular resistance (PVR) → right ventricular strain
Right-to-left shunting on color Doppler = severe PH with hemodynamic compromise
RV dysfunction = poor prognosis, high mortality
Clinical Pearl
Bedside echocardiography can be performed within minutes in the NICU, allowing rapid assessment and guiding escalation to inhaled nitric oxide (iNO) therapy, which is the cornerstone of PH management in MAS.
Why Echocardiography Is Superior
Non-invasive: No radiation, no catheterization risk
Real-time assessment: Can be repeated serially to monitor response to therapy
Functional information: Assesses RV contractility and shunt direction, not just pressure estimates
Guides therapy: Presence of severe PH with right-to-left shunting is an indication for iNO
Why Other Options Are Incorrect
Cardiac catheterization: Invasive, carries risk of perforation and arrhythmia in neonates. Reserved for cases where non-invasive assessment is inconclusive or for therapeutic intervention (e.g., balloon atrial septostomy in refractory cases). Not first-line.
Pulmonary function testing: Not feasible in acutely ill neonates and does not assess cardiac function or estimate pulmonary artery pressure.
CT chest: Exposes the neonate to significant radiation and requires transport out of the NICU. Not indicated for acute assessment of PH; reserved for ruling out structural lung disease in stable patients.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.